

Placental findings in singleton stillbirths
- PMID: 24402599
- PMCID: PMC3948332
- DOI: 10.1097/AOG.0000000000000100
Placental findings in singleton stillbirths
Abstract
Objective: To compare placental lesions for stillbirth cases and live birth controls in a population-based study.
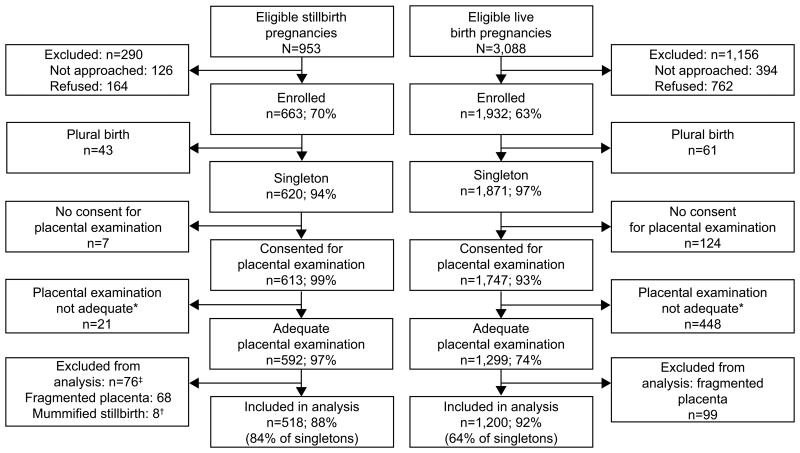
Methods: Pathologic examinations were performed on placentas from singleton pregnancies using a standard protocol. Data were analyzed overall and within gestational age groups at delivery.
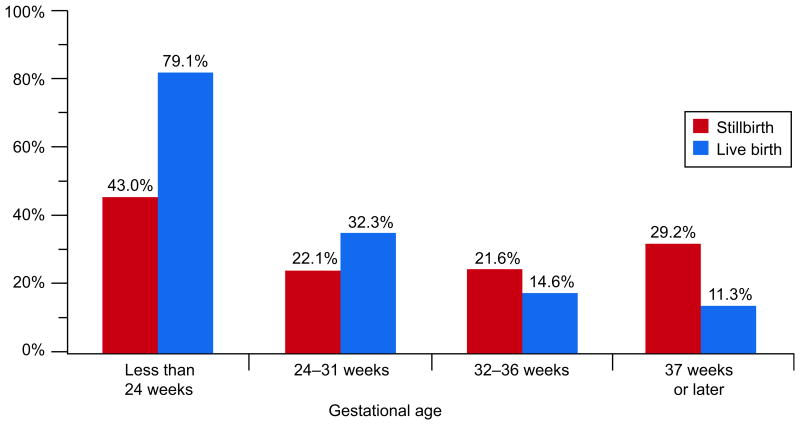
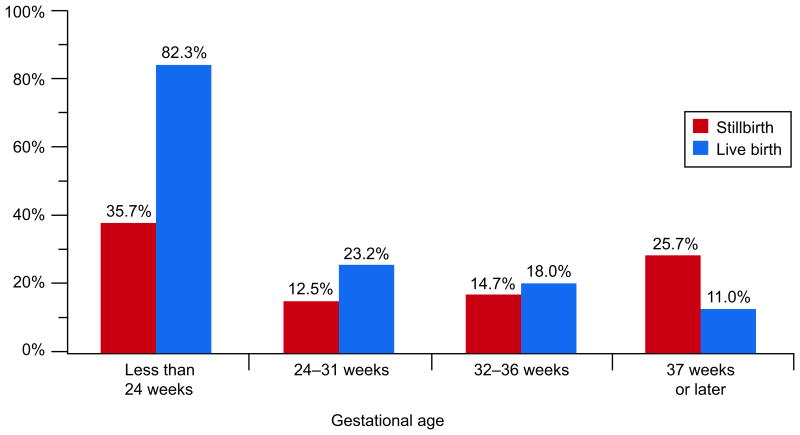
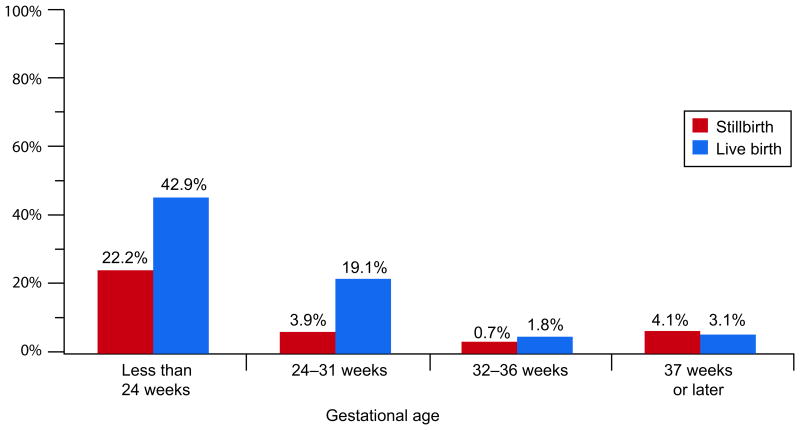
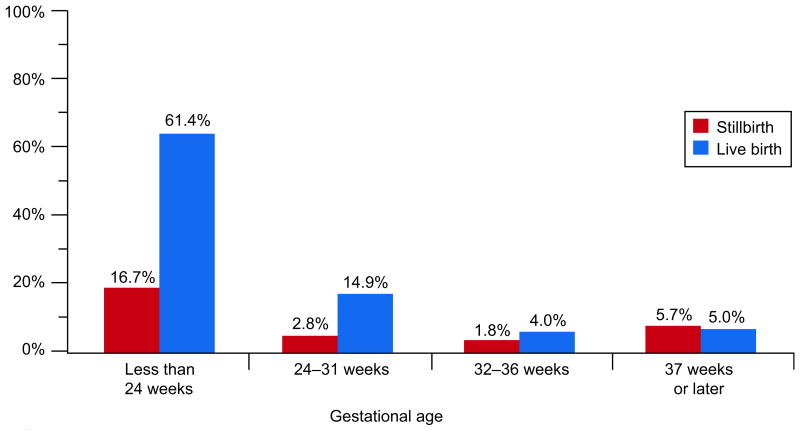
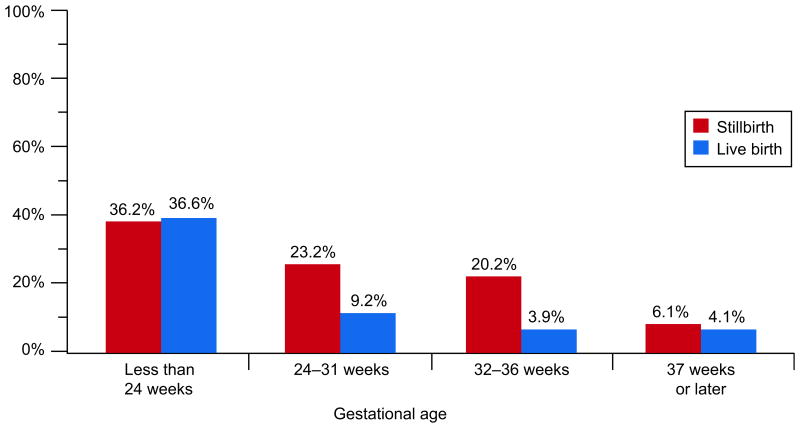
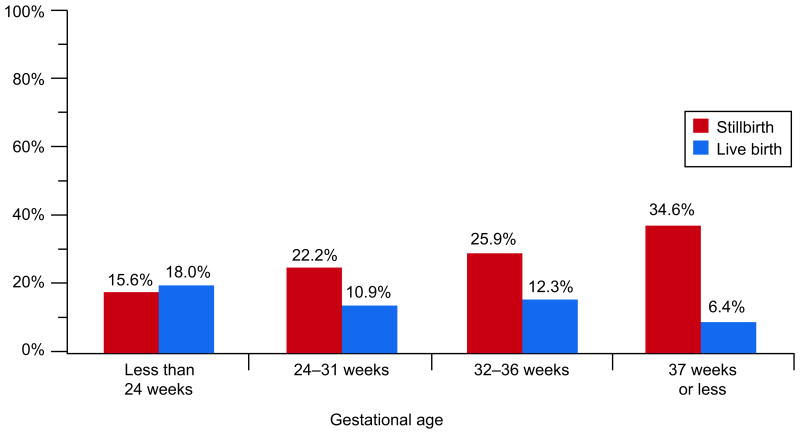
Results: Placentas from 518 stillbirths and 1,200 live births were studied. Single umbilical artery was present in 7.7% of stillbirths and 1.7% of live births, velamentous cord insertion was present in 5% of stillbirths and 1.1% of live births, diffuse terminal villous immaturity was present in 10.3% of stillbirths and 2.3% of live births, inflammation (eg, acute chorioamnionitis of placental membranes) was present in 30.4% of stillbirths and 12% of live births, vascular degenerative changes in chorionic plate were present in 55.7% of stillbirths and 0.5% of live births, retroplacental hematoma was present in 23.8% of stillbirths and 4.2% of live births, intraparenchymal thrombi was present in 19.7% of stillbirths and 13.3% of live births, parenchymal infarction was present in 10.9% of stillbirths and 4.4% of live births, fibrin deposition was present in 9.2% of stillbirths and 1.5% of live births, fetal vascular thrombi was present in 23% of stillbirths and 7% of live births, avascular villi was present in 7.6% of stillbirths and 2.0% of live births, and hydrops was present in 6.4% of stillbirths and 1.0% of live births. Among stillbirths, inflammation and retroplacental hematoma were more common in placentas from early deliveries, whereas thrombotic lesions were more common in later gestation. Inflammatory lesions were especially common in early live births.
Conclusions: Placental lesions were highly associated with stillbirth compared with live births. All lesions associated with stillbirth were found in live births but often with variations by gestational age at delivery. Knowledge of lesion prevalence within gestational age groups in both stillbirths and live birth controls contributes to an understanding of the association between placental abnormality and stillbirth.
Level of evidence: II.
Figures
References
-
- Graafmans WC, Richardus JH, Macfarlane A, et al. EuroNatal Working Group. Comparability of published perinatal mortality rates in Western Europe: the quantitative impact of differences in gestational age and birthweight criteria. BJOG. 2001;108(12):1237–1245. - PubMed
-
- MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep. 2009;57(8):1–19. - PubMed
-
- Cousens S, Blencowe H, Stanton C, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet. 2011;377(9774):1319–1330. - PubMed
-
- Saller DN, Jr, Lesser KB, Harrel U, Rogers BB, Oyer CE. The clinical utility of the perinatal autopsy. JAMA. 1995 Feb 22;273(8):663–5. - PubMed
-
- Faye-Petersen OM, Guinn DA, Wenstrom KD. Value of perinatal autopsy. Obstet Gynecol. 1999;94(6):915–920. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
