

Bone density and fractures in autosomal dominant hyper IgE syndrome
- PMID: 24402620
- PMCID: PMC4484798
- DOI: 10.1007/s10875-013-9982-2
Bone density and fractures in autosomal dominant hyper IgE syndrome
Abstract
Purpose: Autosomal Dominant Hyper IgE Recurrent Infection Syndrome (AD-HIES) is caused by mutations in STAT3 and characterized by eczema, recurrent bacterial infections, and skeletal and connective tissue abnormalities. To further understand the minimal trauma fractures of AD-HIES, we examined bone mineral density (BMD) and laboratory markers of bone turnover.
Methods: Patients with AD-HIES enrolled in a prospective natural history study were examined with dual x-ray absorptiometry (DEXA) scans and laboratory studies of bone metabolism. The number of fractures was recorded as well as clinical features of AD-HIES including scoliosis and retained primary teeth. Patients on medications with skeletal effects, including bisphosphonates, were examined separately.
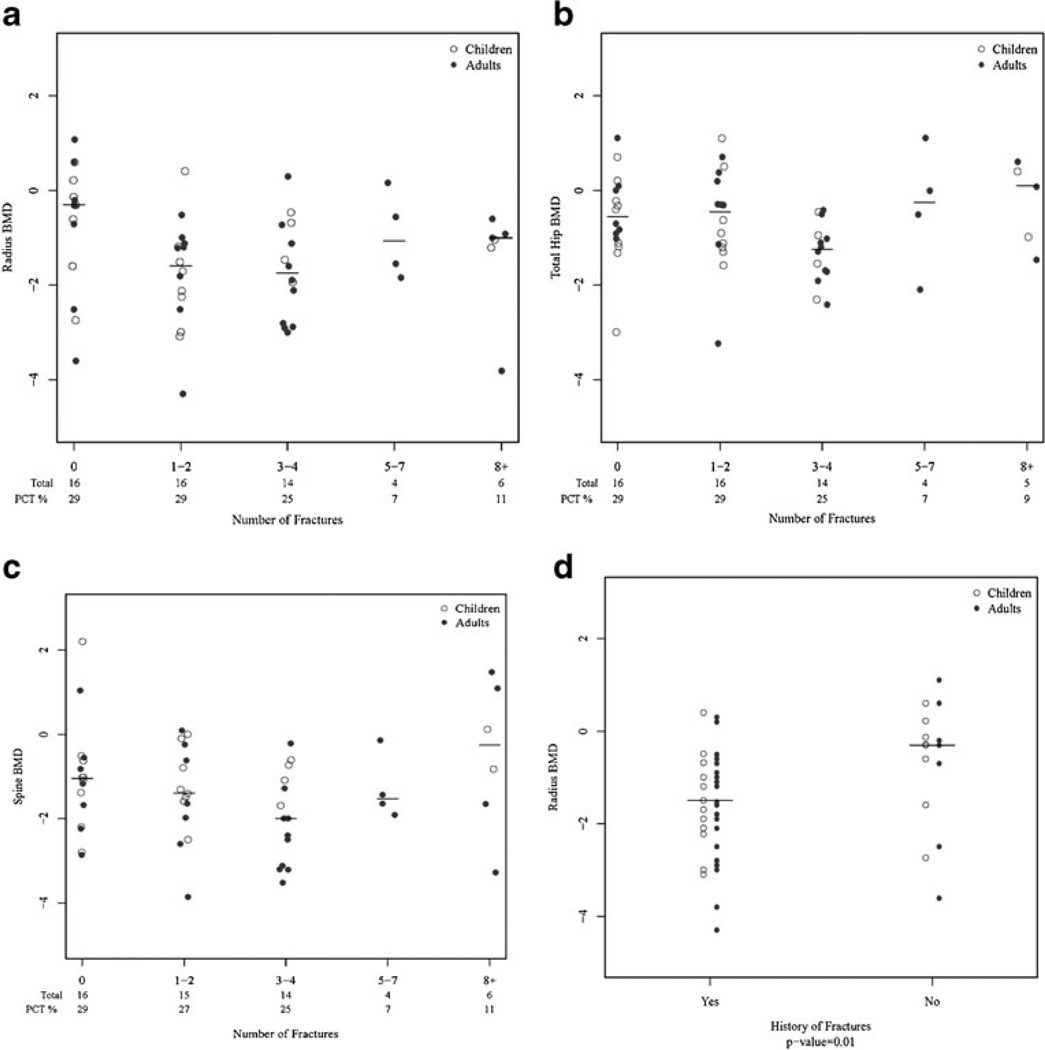
Results: Twenty-three AD-HIES children (6-18 years) and 33 AD-HIES adults (21-50 years) not receiving bone-active drugs were studied. Fourteen of the 23 children (61%) had histories of minimal trauma fractures, as did 26 of the 33 adults (79%). Osteopenia or osteoporosis was found in 79% of children and adults. Only radial BMD correlated with the qualitative occurrence of fractures but it did not correlate with the numbers of fractures. Markers of bone metabolism did not correlate with minimal trauma fractures or BMD. Patients on bone-active medications had improved BMD, but still sustained fractures.
Conclusions: Minimal trauma fractures and decreased BMD are common in AD-HIES. Low radial BMD is associated with fractures, but hip and spine BMD are not. Treatment with bisphosphonates increased BMD but its role in fracture prevention remains undefined.
Figures
References
-
- Minegishi Y, Saito M, Tsuchiya S, Tsuge I, Takada H, Hara T, et al. Dominant-negative mutations in the DNA-binding domain of STAT3 cause hyper-IgE syndrome. Nature. 2007;448(7157):1058–1062. Research Support, Non-U.S. Gov’t. - PubMed
-
- Buckley RH, Wray BB, Belmaker EZ. Extreme hyperimmunoglobulinemia E and undue susceptibility to infection. Pediatrics. 1972;49(1):59–70. In Vitro. - PubMed
-
- Holland SM, DeLeo FR, Elloumi HZ, Hsu AP, Uzel G, Brodsky N, et al. STAT3 mutations in the hyper-IgE syndrome. N Engl J Med. 2007;357(16):1608–1619. Research Support, N.I.H., Extramural Research Support, N.I.H., Intramural Research Support, Non-U.S. Gov’t. - PubMed
-
- Grimbacher B, Holland SM, Gallin JI, Greenberg F, Hill SC, Malech HL, et al. Hyper-IgE syndrome with recurrent infections—an autosomal dominant multisystem disorder. N Engl J Med. 1999;340(9):692–702. Research Support, Non-U.S. Gov’t. - PubMed
-
- Cohen-Solal M, Prieur AM, Prin L, Denne MA, Launay JM, Graulet AM, et al. Cytokine-mediated bone resorption in patients with the hyperimmunoglobulin E syndrome. Clin Immunol Immunopathol. 1995;76(1 Pt 1):75–81. Comparative Study In Vitro. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
