

Evaluation of Anosognosia in Alzheimer's Disease Using the Symptoms of Early Dementia-11 Questionnaire (SED-11Q)
- PMID: 24403907
- PMCID: PMC3884202
- DOI: 10.1159/000355367
Evaluation of Anosognosia in Alzheimer's Disease Using the Symptoms of Early Dementia-11 Questionnaire (SED-11Q)
Abstract
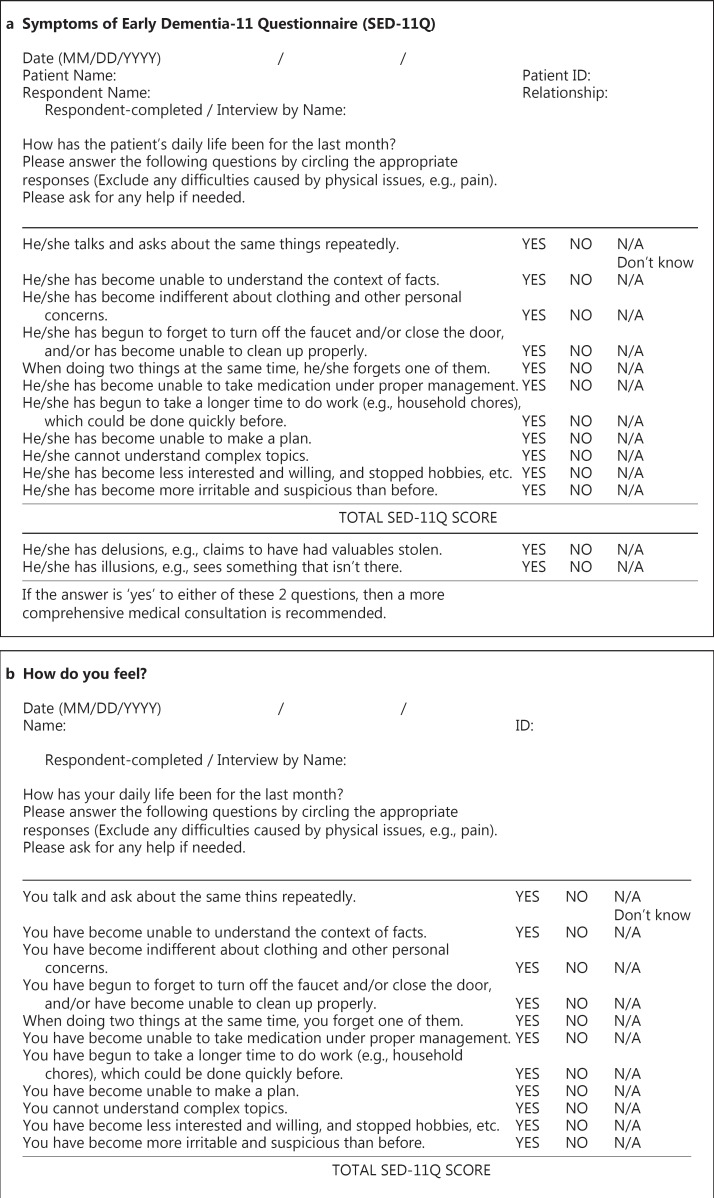
Aims: The objective is to propose a brief method to evaluate anosognosia in Alzheimer's disease (AD) using the Symptoms of Early Dementia-11 Questionnaire (SED-11Q), a short informant-based screening questionnaire for identifying dementia.
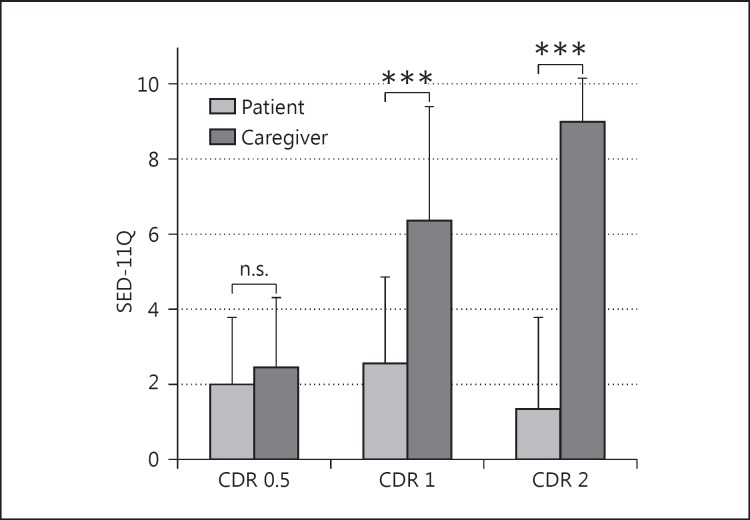
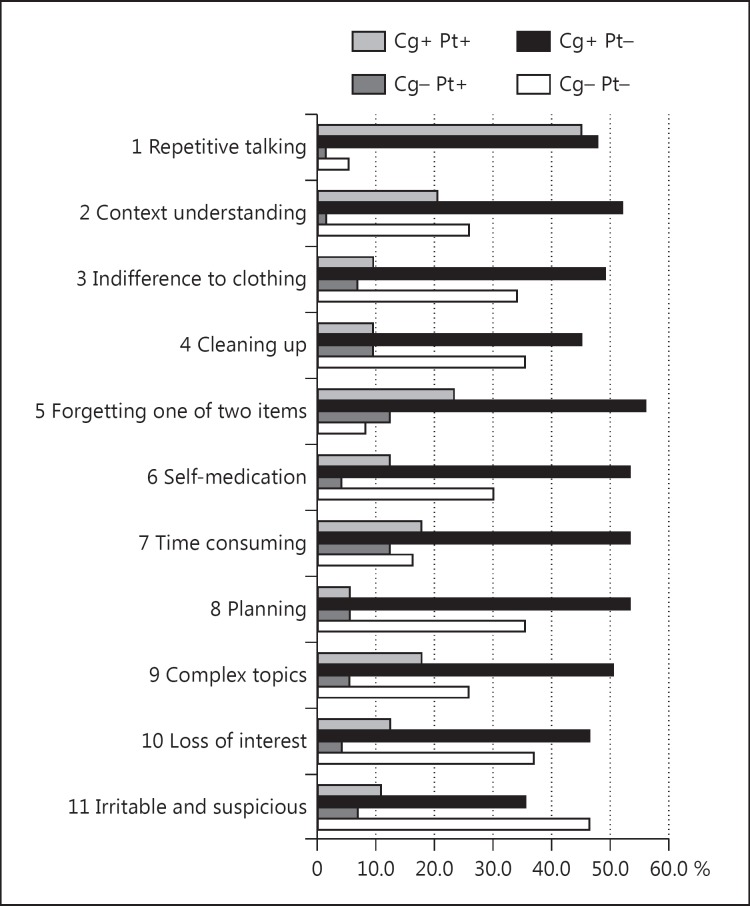
Methods: The participants were 107 elderly individuals: 13 with a Clinical Dementia Rating (CDR) of 0.5, 73 with mild AD of CDR 1, and 21 with moderate AD of CDR 2. The patients and caregivers answered the SED-11Q independently, and the degree of discrepancy indicated the severity of anosognosia.
Results: THE SCORES WERE AS FOLLOWS: caregiver scores were 2.46 ± 1.85 (mean ± SD) in CDR 0.5, 6.36 ± 3.02 in CDR 1, and 9.00 ± 1.14 in CDR 2; patient scores were 2.00 ± 1.78, 2.55 ± 2.33, and 1.33 ± 2.46, respectively. Discrepancy was 0.46 ± 1.61, 3.81 ± 3.95, and 7.67 ± 2.87, respectively, and the caregiver assessments were significantly higher than the patient assessments in CDR 1 and CDR 2 (p < 0.001 in both groups). The SED-11Q for anosognosia was validated with the standardized Anosognosia Questionnaire for Dementia (AD-Q). The caregiver scores were moderately correlated with behavioral and psychological symptoms of dementia scores (r = 0.524), and the patient scores were moderately correlated with depression scores (r = 0.561).
Conclusion: The SED-11Q serves a dual purpose: caregiver assessment is useful for the screening of dementia, and any discrepancy between the patient and the caregiver assessment is considered as an indication of the severity of anosognosia; this can be informative for caregivers and essential for successful care.
Keywords: Alzheimer's disease; Anosognosia; Behavioral and psychological symptoms of dementia; Caregiver burden; Dementia; Dementia care; Metacognition; Mild cognitive impairment; Screening test.
Figures
References
-
- Starkstein SE, Chemerinski E, Sabe L, Kuzis G, Petracca G, Teson A, Leiguarda R. Prospective longitudinal study of depression and anosognosia in Alzheimer's disease. Br J Psychiatry. 1997;171:47–52. - PubMed
-
- Vasterling JJ, Seltzer B, Watrous WE. Longitudinal assessment of deficit unawareness in Alzheimer's disease. Neuropsychiatry Neuropsychol Behav Neurol. 1997;10:197–202. - PubMed
-
- Salmon E, Ruby P, Perani D, Kalbe E, Laureys S, Adam S, Collette F. Two aspects of impaired consciousness in Alzheimer's disease. Prog Brain Res. 2005;150:287–298. - PubMed
-
- Clare L, Markova I, Verhey F, Kenny G. Awareness in dementia: a review of assessment methods and measures. Aging Ment Health. 2005;9:394–413. - PubMed
-
- Kashiwa Y, Kitabayashi Y, Narumoto J, Nakamura K, Ueda H, Fukui K. Anosognosia in Alzheimer's disease: association with patient characteristics, psychiatric symptoms and cognitive deficits. Psychiatry Clin Neurosci. 2005;59:697–704. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
