

Danger points, complications and medico-legal aspects in endoscopic sinus surgery
- PMID: 24403974
- PMCID: PMC3884541
- DOI: 10.3205/cto000098
Danger points, complications and medico-legal aspects in endoscopic sinus surgery
Abstract
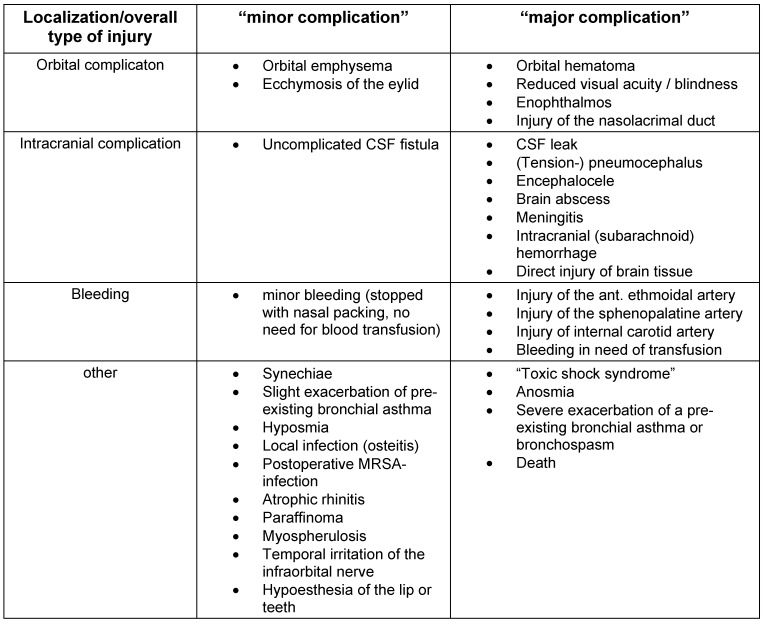
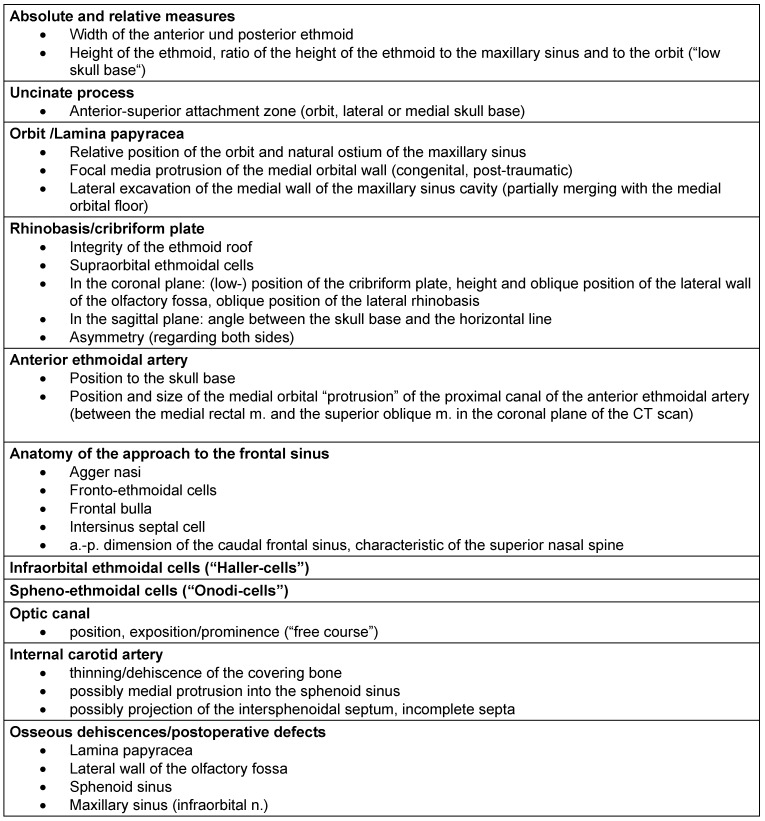
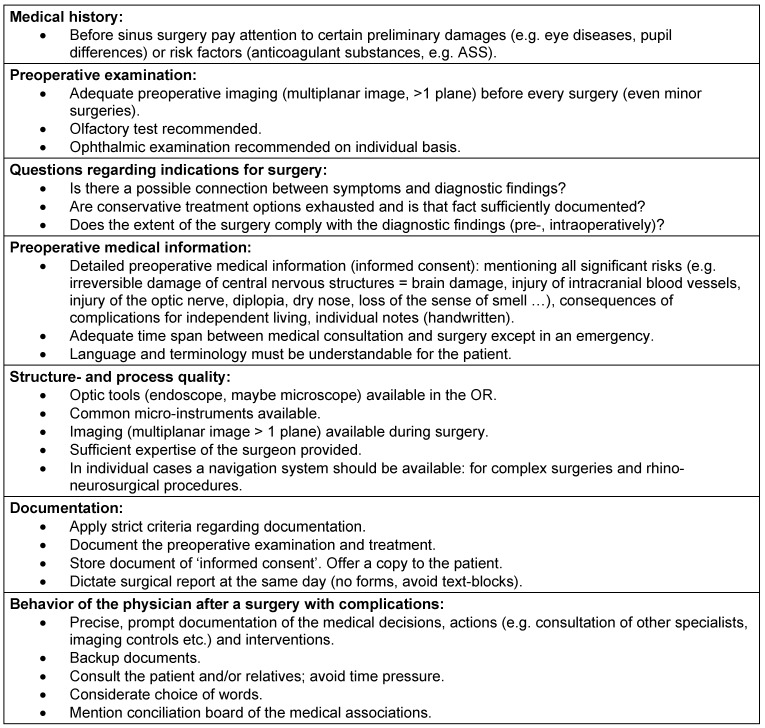
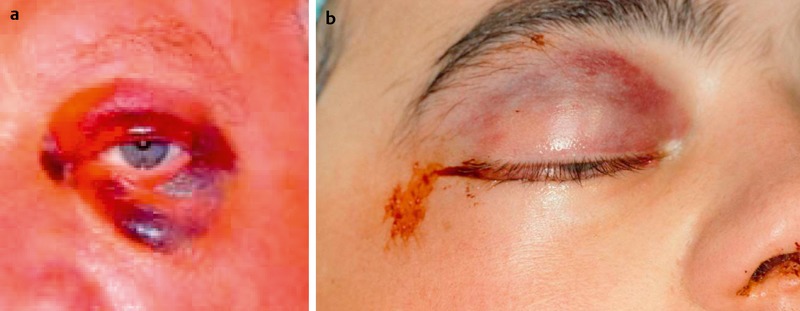
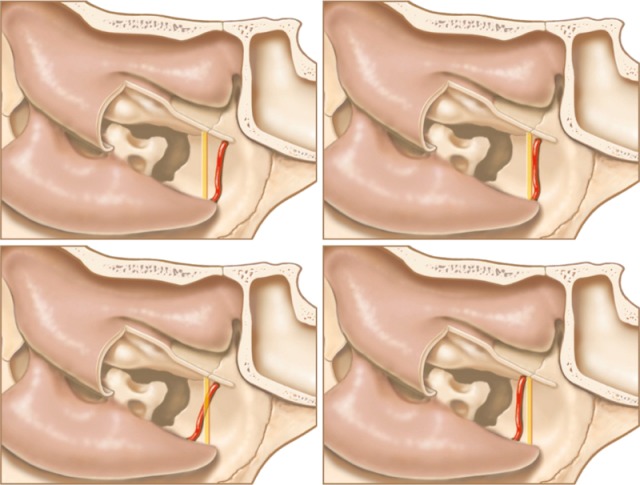
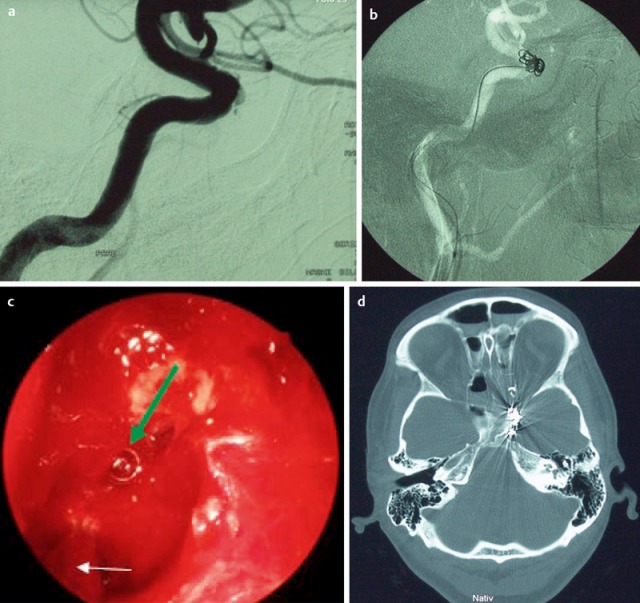
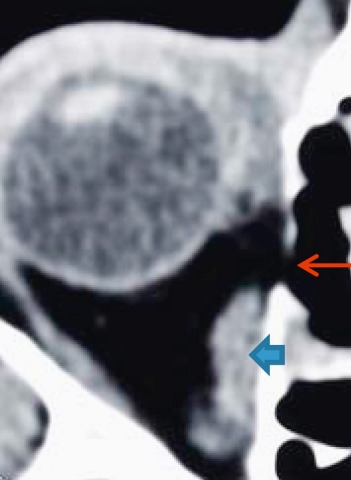
Endoscopic endonasal sinus surgery represents the overall accepted type of surgical treatment for chronic rhinosinusitis. Notwithstanding raised and still evolving quality standards, surgeons performing routine endoscopic interventions are faced with minor complications in 5% and major complications in 0.5-1%. A comprehensive review on all minor and major complications of endoscopic surgery of the paranasal sinuses and also on the anterior skull base is presented listing the actual scientific literature. The pathogenesis, signs and symptoms of each complication are reviewed and therapeutic regimens are discussed in detail relating to actual publication references. Potential medico-legal aspects are explicated and recent algorithms of avoidance are mentioned taking into account options in surgical training and education.
Keywords: FESS; complications; endoscopic sinus surgery; medico-legal aspects; review; skull base surgery.
Figures



References
-
- Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in Canadians. Laryngoscope. 2003 Jul;113(7):1199–1205. doi: 10.1097/00005537-200307000-00016. Available from: http://dx.doi.org/10.1097/00005537-200307000-00016. - DOI - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, Cohen N, Cervin A, Douglas R, Gevaert P, Georgalas C, Goossens H, Harvey R, Hellings P, Hopkins C, Jones N, Joos G, Kalogjera L, Kern B, Kowalski M, Price D, Riechelmann H, Schlosser R, Senior B, Thomas M, Toskala E, Voegels R, Wang de Y, Wormald PJ. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(Suppl 23):1–299. Available from: http://www.rhinologyjournal.com/supplement_23.pdf. - PubMed
-
- Hedman J, Kaprio J, Poussa T, Nieminen MM. Prevalence of asthma, aspirin intolerance, nasi polyposis and chronic obstruction pulmonary disease in a population-based study. Int J Epidemiology. 1999;28:717–722. doi: 10.1093/ije/28.4.717. Available from: http://dx.doi.org/10.1093/ije/28.4.717. - DOI - PubMed
-
- Stuck BA, Bachert C, Federspil P, Hosemann W, Klimek L, Mösges R, Pfaar O, Rudack C, Sitter H, Wagenmann M, Weber R, Hörmann K German Society of Otorhinolaryngology, Head and Neck Surgery. Leitlinie "Rhinosinusitis"--Langfassung: S2-Leitlinie der Deutschen Gesellschaft für Hals-Nasen-Ohren-Heilkunde, Kopf- und Hals-Chirurgie. [Rhinosinusitis guidelines--unabridged version: S2 guidelines from the German Society of Otorhinolaryngology, Head and Neck Surgery]. HNO. 2012 Feb;60(2):141–162. doi: 10.1007/s00106-011-2396-7. (Ger). Available from: http://dx.doi.org/10.1007/s00106-011-2396-7. - DOI - PubMed
-
- Mattos JL, Woodard CR, Payne SC. Trends in common rhinologic illnesses: analysis of U.S. healthcare surveys 1995-2007. Int Forum Allergy Rhinol. 2011 Jan-Feb;1(1):3–12. doi: 10.1002/alr.20003. Available from: http://dx.doi.org/10.1002/alr.20003. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
