

Effects of Methylprednisolone Pulse Therapy on Refractory Mycoplasma pneumoniae Pneumonia in Children
- PMID: 24404389
- PMCID: PMC3881395
- DOI: 10.4168/aair.2014.6.1.22
Effects of Methylprednisolone Pulse Therapy on Refractory Mycoplasma pneumoniae Pneumonia in Children
Abstract
Purpose: Mycoplasma pneumoniae (M. pneumoniae) is one of the most common causes of community-acquired pneumonia in children. The clinical course is typically self-limited and benign; however, rare cases of severe pneumonia can develop despite appropriate antibiotic therapy. We studied the effects of methylprednisolone pulse therapy on severe refractory M. pneumoniae pneumonia in children.
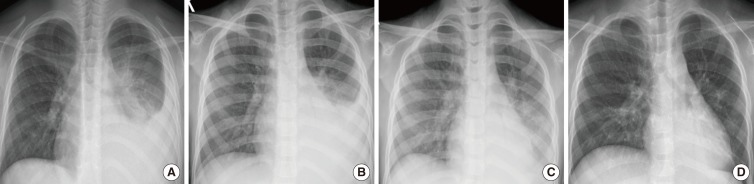
Methods: The clinical effects of methylprednisolone therapy were evaluated retrospectively in 12 children with severe refractory M. pneumoniae pneumonia, which was diagnosed serologically. All patients developed respiratory distress, high fever, and initial lobar pneumonic consolidation based on radiological findings. All clinical symptoms deteriorated despite appropriate antibiotic therapy. Thus, children were treated with intravenous methylprednisolone pulse therapy in addition to antibiotics.
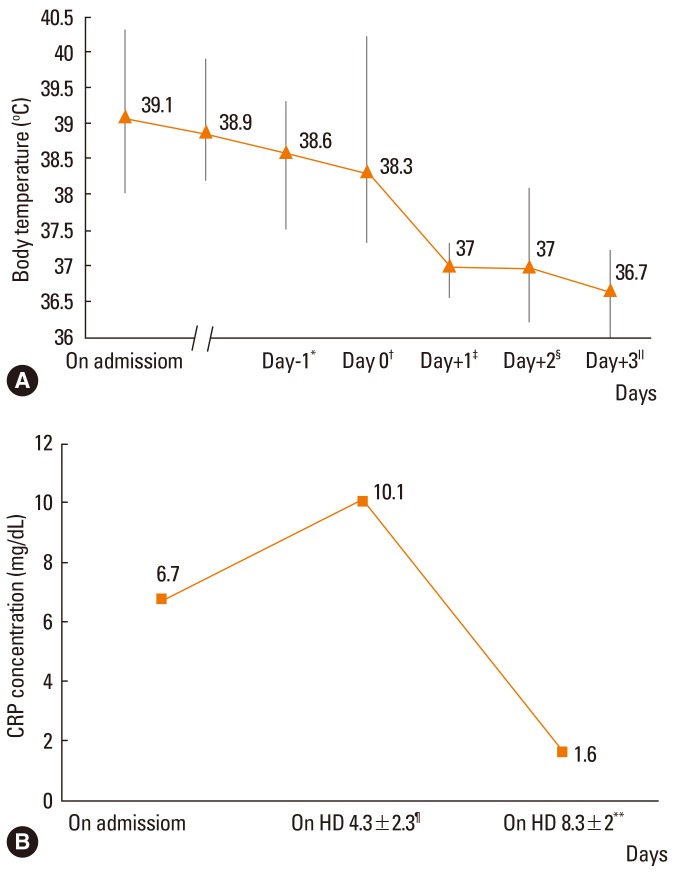
Results: The average febrile period before admission was 4.9±1.7 days, and fever persisted in all children until steroid administration. Methylprednisolone pulse therapy (30 mg/kg) was given 5.4±2.5 days after admission. After methylprednisolone pulse therapy, clinical symptoms improved in all patients without adverse events. The fever subsided 0-2 h after initiation of corticosteroid therapy. The abnormal radiological findings resolved within 2.6±1.3 days, and the high C-reactive protein levels (6.7±5.9 mg/dL) on admission decreased to 1.3±1.7 mg/dL within 3.0±1.1 days after starting corticosteroid therapy.
Conclusions: Three-day methylprednisolone pulse therapy could be applied to treatment of refractory M. pneumoniae pneumonia despite appropriate antibiotic therapy and appeared to be efficacious and well-tolerated.
Keywords: Children; Mycoplasma pneumoniae; methylprednisolone; pneumonia.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
References
-
- Atkinson TP, Balish MF, Waites KB. Epidemiology, clinical manifestations, pathogenesis and laboratory detection of Mycoplasma pneumoniae infections. FEMS Microbiol Rev. 2008;32:956–973. - PubMed
-
- Heiskanen-Kosma T, Korppi M, Jokinen C, Kurki S, Heiskanen L, Juvonen H, Kallinen S, Stén M, Tarkiainen A, Rönnberg PR, Kleemola M, Mäkelä PH, Leinonen M. Etiology of childhood pneumonia: serologic results of a prospective, population-based study. Pediatr Infect Dis J. 1998;17:986–991. - PubMed
-
- Sinaniotis CA, Sinaniotis AC. Community-acquired pneumonia in children. Curr Opin Pulm Med. 2005;11:218–225. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
