

Use of secondary prevention pharmacotherapy after first myocardial infarction in patients with diabetes mellitus
- PMID: 24406095
- PMCID: PMC3897983
- DOI: 10.1186/1471-2261-14-4
Use of secondary prevention pharmacotherapy after first myocardial infarction in patients with diabetes mellitus
Abstract
Background: Despite recommended pharmacotherapies the use of secondary prevention therapy after myocardial infarction (MI) remains suboptimal. Patients with diabetes mellitus (DM) have worse prognosis after MI compared to patients without DM and aggressive secondary prevention pharmacotherapy in this population is therefore warranted. We examined the changes in use of evidence-based secondary prevention pharmacotherapy in patients with and without DM discharged after first MI.
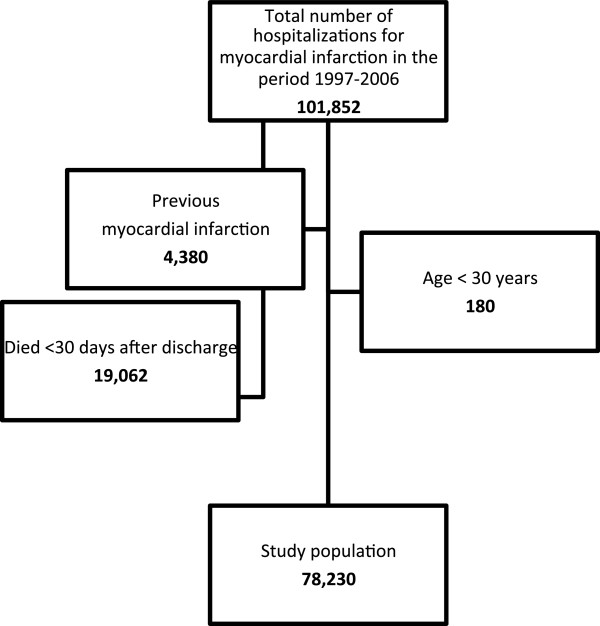
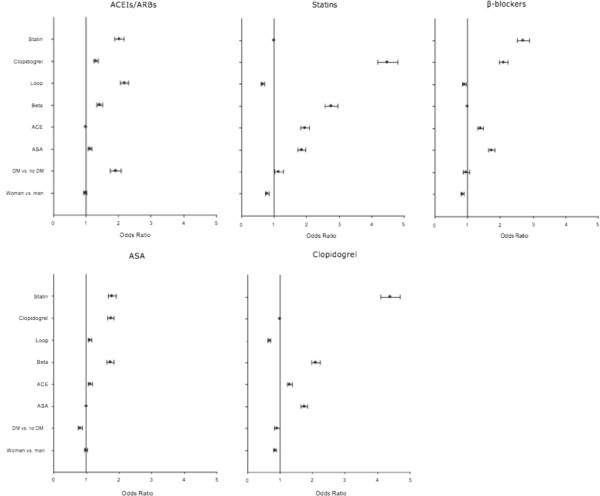
Methods: All patients aged 30 years or older admitted with first MI in Denmark during 1997-2006 were identified by individual-level linkage of nationwide registries of hospitalizations. Univariate and multivariate logistic regression models were used to identify patient characteristics associated with initiation of acetylsalicylic acid, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, β-blockers, and clopidogrel within 90 days, and statins within 180 days of discharge, respectively.
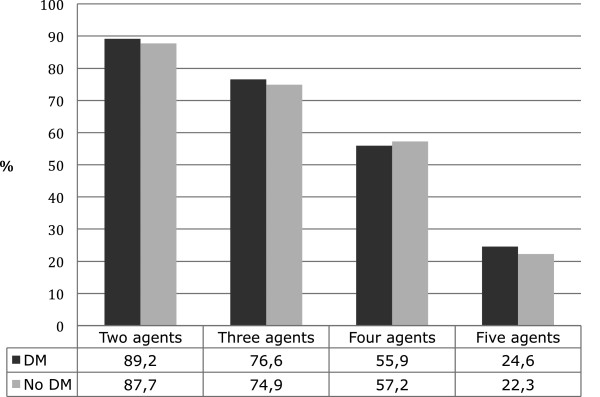
Results: A total of 78,230 patients were included, the mean age was 68.3 years (SD 13.0), 63.5% were men and 9,797 (12.5%) had diabetes. Comparison of claimed prescriptions in the period 1997-2002 and 2003-2006 showed significant (p < 0.001) increases in claims for acetylsalicylic acid (38.9% vs. 69.7%), angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (38.7% vs. 50.4%), β-blockers (69.2% vs. 77.9%), clopidogrel (16.7% vs. 66.3%), and statins (41.3% vs. 77.3%). During 2003-2006, patients with DM claimed significantly less acetylsalicylic acid (odds ratio [OR] 0.81 [95% confidence interval [CI] 0.74-0.88) and clopidogrel (OR 0.91 [95% CI 0.83-1.00]) than patients without DM.
Conclusions: Despite sizeable increase in use of evidence-based secondary prevention pharmacotherapy after MI from 1997 to 2006, these drugs are not used in a substantial proportion of subjects and patients with DM received significantly less antiplatelet therapy than patients without DM. Increased focus on initiation of secondary prevention pharmacotherapy after MI is warranted, especially in patients with DM.
Figures
Similar articles
-
Adherence to recommendations for secondary prevention medications after myocardial infarction in Estonia: comparison of real-world data from 2004 to 2005 and 2017 to 2018.BMC Cardiovasc Disord. 2021 Oct 20;21(1):505. doi: 10.1186/s12872-021-02321-x. BMC Cardiovasc Disord. 2021. PMID: 34670499 Free PMC article.
-
Guideline-recommended secondary prevention drug therapy after acute myocardial infarction: predictors and outcomes of nonadherence.Eur J Cardiovasc Prev Rehabil. 2010 Oct;17(5):576-81. doi: 10.1097/HJR.0b013e328338e5da. Eur J Cardiovasc Prev Rehabil. 2010. PMID: 20351550
-
Chronic polytherapy after myocardial infarction: the trade-off between hospital and community-based providers in determining adherence to medication.BMC Cardiovasc Disord. 2021 Apr 14;21(1):180. doi: 10.1186/s12872-021-01969-9. BMC Cardiovasc Disord. 2021. PMID: 33853534 Free PMC article.
-
Lack of efficacy of drug therapy in preventing takotsubo cardiomyopathy recurrence: a meta-analysis.Clin Cardiol. 2014 Jul;37(7):434-9. doi: 10.1002/clc.22280. Epub 2014 Apr 3. Clin Cardiol. 2014. PMID: 24700369 Free PMC article. Review.
-
Secondary Prevention after Myocardial Infarction: What to Do and Where to Do It.Rev Cardiovasc Med. 2022 Jun 8;23(6):210. doi: 10.31083/j.rcm2306210. eCollection 2022 Jun. Rev Cardiovasc Med. 2022. PMID: 39077194 Free PMC article. Review.
Cited by
-
Time trends in statin use and incidence of recurrent cardiovascular events in secondary prevention between 1999 and 2013: a registry-based study.BMC Cardiovasc Disord. 2018 Nov 6;18(1):209. doi: 10.1186/s12872-018-0941-y. BMC Cardiovasc Disord. 2018. PMID: 30400778 Free PMC article.
-
Determinants of angiotensin-converting enzyme inhibitor (ACEI) intolerance and angioedema in the UK Clinical Practice Research Datalink.Br J Clin Pharmacol. 2016 Dec;82(6):1647-1659. doi: 10.1111/bcp.13090. Epub 2016 Oct 4. Br J Clin Pharmacol. 2016. PMID: 27524468 Free PMC article.
-
Gender disparity in the prescription of secondary prevention medications in a Malaysian primary care clinic.Malays Fam Physician. 2021 Jun 8;16(2):37-44. doi: 10.51866/oa1080. eCollection 2021 Jul 22. Malays Fam Physician. 2021. PMID: 34386162 Free PMC article.
-
Outcomes in CME/CPD - Special Collection: How to make the "pyramid" a perpetuum mobile.J Eur CME. 2020 Oct 27;9(1):1832750. doi: 10.1080/21614083.2020.1832750. J Eur CME. 2020. PMID: 33194316 Free PMC article.
-
Substitution of red meat with soybean but not non- soy legumes improves inflammation in patients with type 2 diabetes; a randomized clinical trial.J Diabetes Metab Disord. 2018 Aug 17;17(2):111-116. doi: 10.1007/s40200-018-0346-6. eCollection 2018 Dec. J Diabetes Metab Disord. 2018. PMID: 30918843 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
