

Tricyclic antidepressants for management of residual symptoms in inflammatory bowel disease
- PMID: 24406434
- PMCID: PMC4111227
- DOI: 10.1097/MCG.0000000000000049
Tricyclic antidepressants for management of residual symptoms in inflammatory bowel disease
Abstract
Background: Tricyclic antidepressants (TCAs) have efficacy in treating irritable bowel syndrome (IBS). Some clinicians use TCAs to treat residual symptoms in inflammatory bowel disease (IBD) patients already on decisive IBD therapy or with quiescent inflammation, although this strategy has not been formally studied.
Goals: The aim of this study was to examine the efficacy of TCA therapy in IBD patients with residual symptoms, despite controlled inflammation, in a retrospective cohort study.
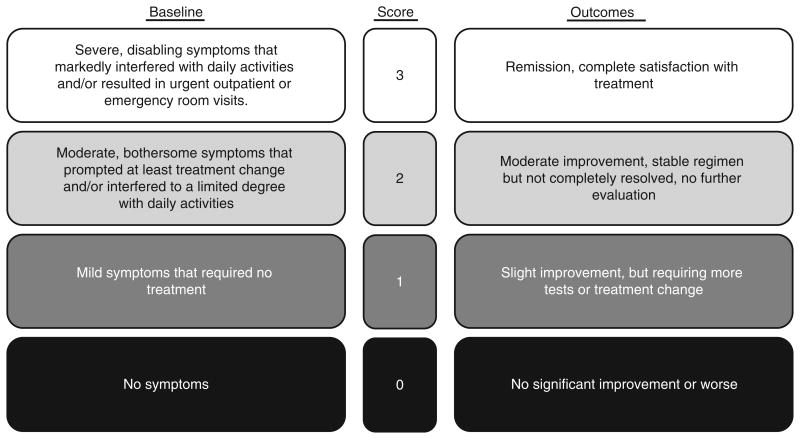
Study: Inclusion required initiation of TCA for persistent gastrointestinal symptoms. IBD patients had inactive or mildly active disease with persistent symptoms despite adequate IBD therapy as determined by their physician. Symptom response was compared with IBS patients. Established Likert scales were used to score baseline symptom severity (0=no symptoms, 3=severe symptoms) and TCA response (0=no improvement; 3=complete satisfaction).
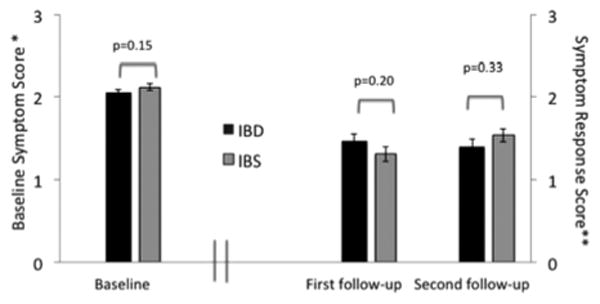
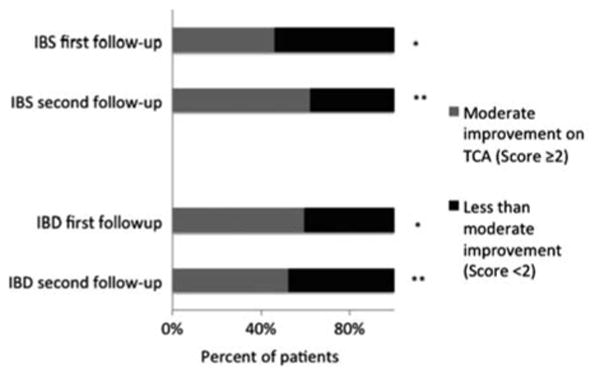
Results: Eighty-one IBD [41.3±1.7 y, 56F; 58 Crohn's disease/23 ulcerative colitis (UC)] and 77 IBS (46.2±1.7 y, 60F) patients were initiated on a TCA therapy. Baseline symptom scores (IBD, 2.06±0.03; IBS, 2.12±0.04; P=0.15) and symptom response to TCA therapy (IBD, 1.46±0.09; IBS, 1.30±0.09; P=0.2) were similar in both the groups. At least moderate improvement (Likert score ≥2) on TCA was achieved by comparable proportions of patients (59.3% IBD vs. 46% IBS; P=0.09). Within IBD, response was better with UC than Crohn's disease (1.86±0.13 vs. 1.26±0.11, respectively, P=0.003).
Conclusions: In a clinical practice setting, TCA use led to moderate improvement of residual gastrointestinal symptoms in IBD patients for whom escalation of IBD therapy was not planned. UC patients demonstrated higher therapeutic success. IBD symptom responses were similar to IBS patients.
Figures
Comment in
-
Should FODMAP withdrawal be tried in inflammatory bowel disease patients with irritable bowel syndrome?J Clin Gastroenterol. 2014 May-Jun;48(5):393-4. doi: 10.1097/MCG.0000000000000127. J Clin Gastroenterol. 2014. PMID: 24705090 No abstract available.
-
Treatment of residual inflammatory bowel disease symptoms with low-dose tricyclic antidepressants: why not?J Clin Gastroenterol. 2014 May-Jun;48(5):390-2. doi: 10.1097/MCG.0000000000000098. J Clin Gastroenterol. 2014. PMID: 24714103 No abstract available.
References
-
- Meng J, Agrawal A, Whorwell PJ. Refractory inflammatory bowel disease-could it be an irritable bowel? Nat Rev Gastro-enterol Hepatol. 2013;10:58–61. - PubMed
-
- Simren M, Axelsson J, Gillberg R, et al. Quality of life in inflammatory bowel disease in remission: the impact of IBS-like symptoms and associated psychological factors. Am J Gastroenterol. 2002;97:389–396. - PubMed
-
- Keohane J, O'Mahony C, O'Mahony L, et al. Irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease: a real association or reflection of occult inflammation? Am J Gastroenterol. 2010;105:1788, 1789–1794. quiz 1795. - PubMed
-
- Halpin SJ, Ford AC. Prevalence of symptoms meeting criteria for irritable bowel syndrome in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2012;107:1474–1482. - PubMed
-
- Long MD, Drossman DA. Inflammatory bowel disease, irritable bowel syndrome, or what?: a challenge to the functional-organic dichotomy. Am J Gastroenterol. 2010;105:1796–1798. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
