

The optimal timing of post-prostate biopsy magnetic resonance imaging to guide nerve-sparing surgery
- PMID: 24407179
- PMCID: PMC3955341
- DOI: 10.4103/1008-682X.122190
The optimal timing of post-prostate biopsy magnetic resonance imaging to guide nerve-sparing surgery
Abstract
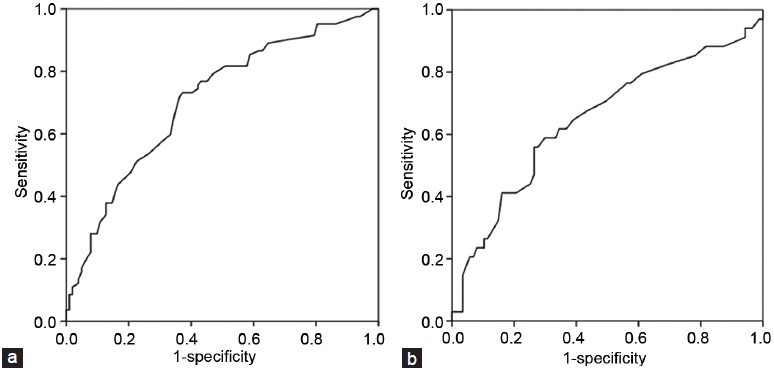
The goal of our study was to evaluate the impact of the interval between prostate biopsy and magnetic resonance imaging (MRI) on the accuracy of simple tumor localization, which is essential information that enables nerve-sparing surgery. We also sought to determine the optimal timing of a post-biopsy MRI. A total of 184 patients who had undergone MRI before radical prostatectomy at an institution without a predetermined schedule for MRI after a prostate biopsy were enrolled. The mean interval from the biopsy to the MRI was 30.8 ± 18.6 days. The accuracy of the MRI for simplifi ed tumor location (right, left, bilateral and none) was 44.6%. In the group with discordant pathologic and MRI fi ndings, the most common reason recorded was 'MRI predicted a unilateral lesion, but pathology revealed bilateral lesions' (58.3%), followed by 'MRI predicted no lesion, but pathology revealed the presence of a lesion' (32.0%). Multivariable analysis showed that the discordant group had a shorter interval (25.0 ± 14.3 vs 38.1 ± 20.6 days, P < 0.01) preceding the MRI and a higher rate of hemorrhage as observed by MRI (80.4% vs 54.8%, P < 0.01) in comparison with the accordant group. In receiver operating characteristics analysis, the area under the curve of the MRI interval in accurate prediction of the tumor location was 0.707 (P < 0.001). At the MRI interval's cutoff of 28.5 days, the sensitivity was 73.2% and the specificity was 63.7%. When the MRI was performed within 28 days, the accumulated accuracy was only 26.1% (23/88); however, when it was performed after 28 days, the reversely accumulated accuracy was 61.5% (59/96). These data support a waiting period of at least 4 weeks after a biopsy before performing an MRI for the purposes of surgical refinement.
Figures
References
-
- Bott SR, Kirby RS. Avoidance and management of positive surgical margins before, during and after radical prostatectomy. Prostate Cancer Prostatic Dis. 2002;5:252–63. - PubMed
-
- White S, Hricak H, Forstner R, Kurhanewicz J, Vigneron DB, et al. Prostate cancer: effect of postbiopsy hemorrhage on interpretation of MR images. Radiology. 1995;195:385–90. - PubMed
-
- Schiebler ML, Schnall MD, Pollack HM, Lenkinski RE, Tomaszewski JE, et al. Current role of MR imaging in the staging of adenocarcinoma of the prostate. Radiology. 1993;189:339–52. - PubMed
-
- D’Amico AV, Schnall M, Whittington R, Malkowicz SB, Schultz D, et al. Endorectal coil magnetic resonance imaging identifies locally advanced prostate cancer in select patients with clinically localized disease. Urology. 1998;51:449–54. - PubMed
-
- Sommer FG, Nghiem HV, Herfkens R, McNeal J, Low RN. Determining the volume of prostatic carcinoma: value of MR imaging with an external-array coil. AJR Am J Roentgenol. 1993;161:81–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
