

Bone loss management in total knee revision surgery
- PMID: 24407821
- PMCID: PMC3923937
- DOI: 10.1007/s00264-013-2262-1
Bone loss management in total knee revision surgery
Abstract
Purpose: Bone stock reconstruction in TKR surgery is one of the biggest challenges for the surgeon. According to some, authors causes of bone stock loosening are multiple, including stress shielding, osteolysis from wear, septic or aseptic loosening, and bone loss caused by a poorly balanced implant. Moreover, bone loss may be iatrogenic at the time of implant removal, indicating that bone preservation during implant removal is critical.
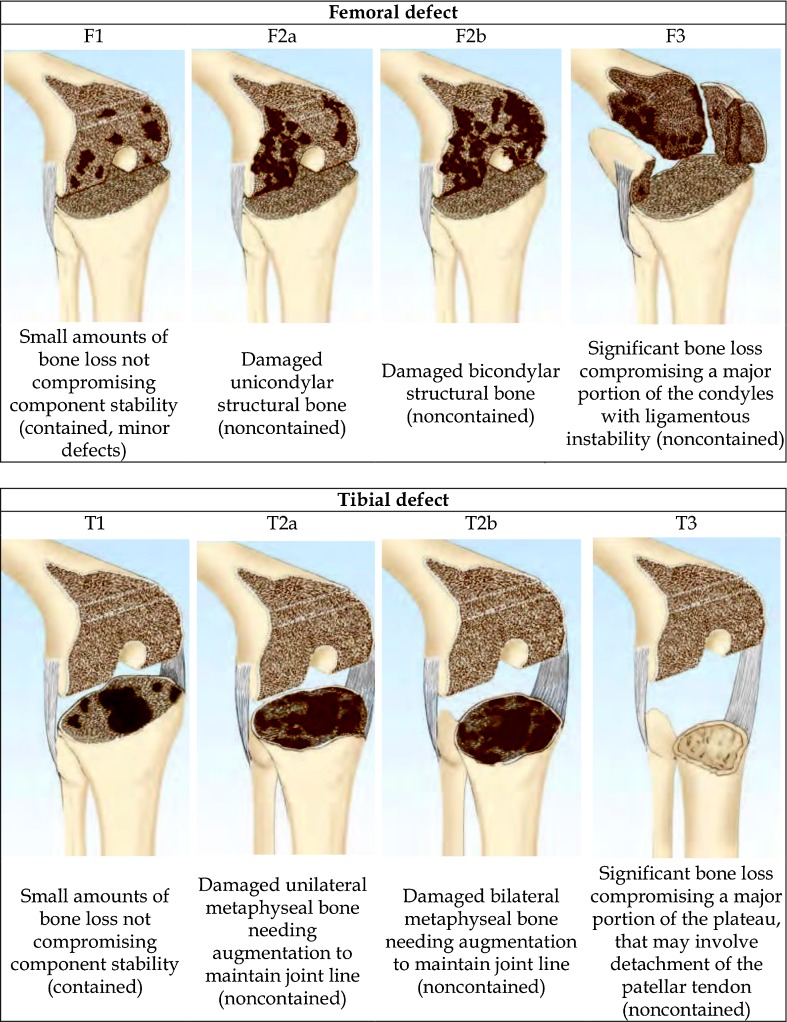
Methods: Defect localization and extension affect the surgeon's decisions about the choice of the surgical technique and the type of plant to be taken. Today there are several options available for bone deficiency treatment. The treatment choice is undoubtedly linked to the cause of revision, experience and personal philosophy, but it is necessary to consider also the patient's age, expectations of life, functional requirements and bone quality. Many authors prefer bone stock reconstruction techniques in patients with high bone quality and a better quality of life with more prospects. In patients with lower lease on life and lower bone quality the best bone replacement techniques are of modular systems, wedges, and augments. In cases with septic bone loss, more or less extended, different authors recommend reducing bone grafts in favor of modular prostheses to reduce the risk of graft contamination.
Results: All of these techniques have been shown to be durable in midterm outcomes, but concerns exist for a number of reasons, including disease transmission, resorption, fracture, immune reaction to allograft, the cost of custom prostheses, the inability to modify the construct intraoperatively and the overall technical challenge of applying these techniques.
Conclusions: The choice between different surgical options depends on bone defect dimension and characteristics but are also patient-related. Reestablishment of well-aligned and stable implants is necessary for successful reconstruction, but this can't be accomplished without a sufficient restoration of an eventual bone loss.
Figures
References
-
- Clatworthy MG, Ballance J, Brick GW, Chandler HP, Gross AE. The use of structural allograft for uncontained defects in revision total knee arthroplasty. A minimum five-year review. J Bone Joint Surg Am. 2001;83-A(3):404–411. - PubMed
-
- Engh GA, Ammen DJ. Bone loss with revision total knee arthroplasty: defect classification and alternatives for reconstruction. Instr Course Lect. 1995;48:167–175. - PubMed
-
- Merchant AC, Mercer RL, Jacobsen RH, Cool CR. Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56(7):1391–1396. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
