

Bowel wall thickening at CT: simplifying the diagnosis
- PMID: 24407923
- PMCID: PMC3999365
- DOI: 10.1007/s13244-013-0308-y
Bowel wall thickening at CT: simplifying the diagnosis
Abstract
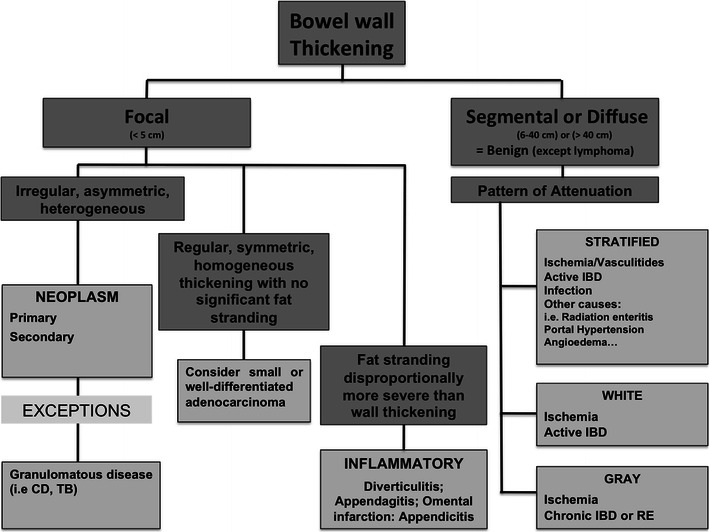
Objective: In this article we present a simplified algorithm-based approach to the thickening of the small and large bowel wall detected on routine computed tomography (CT) of the abdomen.
Background: Thickening of the small or large bowel wall may be caused by neoplastic, inflammatory, infectious, or ischaemic conditions. First, distinction should be made between focal and segmental or diffuse wall thickening. In cases of focal thickening further analysis of the wall symmetry and perienteric anomalies allows distinguishing between neoplasms and inflammatory conditions. In cases of segmental or diffuse thickening, the pattern of attenuation in light of clinical findings helps narrowing the differential diagnosis.
Conclusion: Focal bowel wall thickening may be caused by tumours or inflammatory conditions. Bowel tumours may appear as either regular and symmetric or irregular or asymmetric thickening. When fat stranding is disproportionately more severe than the degree of wall thickening, inflammatory conditions are more likely. With the exception of lymphoma, segmental or diffuse wall thickening is usually caused by benign conditions, such as ischaemic, infectious and inflammatory diseases.
Key points: • Thickening of the bowel wall may be focal (<5 cm) and segmental or diffuse (6-40 cm or >40 cm) in extension. • Focal, irregular and asymmetrical thickening of the bowel wall suggests a malignancy. • Perienteric fat stranding disproportionally more severe than the degree of wall thickening suggests an inflammatory condition. • Regular, symmetric and homogeneous wall thickening is more frequently due to benign conditions, but can also be caused by neoplasms such as well-differentiated adenocarcinoma and lymphoma. • Segmental or diffuse bowel wall thickening is usually caused by ischaemic, inflammatory or infectious conditions and the attenuation pattern is helpful in narrowing the differential diagnosis.
Figures







Similar articles
-
Evaluation of bowel wall thickening by computed tomography to differentiate benign from malignant lesions.J Clin Diagn Res. 2014 Nov;8(11):RC09-12. doi: 10.7860/JCDR/2014/10601.5149. Epub 2014 Nov 20. J Clin Diagn Res. 2014. PMID: 25584284 Free PMC article.
-
Multidetector computed tomography in large bowel lesions-a study of 100 cases.Indian J Surg. 2011 Oct;73(5):352-8. doi: 10.1007/s12262-011-0325-3. Epub 2011 Aug 5. Indian J Surg. 2011. PMID: 23024540 Free PMC article.
-
Pixel to Pathology: A Prospective Cross-Sectional Study on the Role of Multidetector Computed Tomography in the Evaluation of Malignant Large Bowel Lesions With Histopathological Correlation.Cureus. 2024 Oct 10;16(10):e71200. doi: 10.7759/cureus.71200. eCollection 2024 Oct. Cureus. 2024. PMID: 39525180 Free PMC article.
-
CT evaluation of wall thickening in the alimentary tract.Radiographics. 1991 Sep;11(5):771-83; discussion 784. doi: 10.1148/radiographics.11.5.1947313. Radiographics. 1991. PMID: 1947313 Review.
-
Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain.Radiographics. 2004 May-Jun;24(3):703-15. doi: 10.1148/rg.243035084. Radiographics. 2004. PMID: 15143223 Review.
Cited by
-
Treatment of intestinal tuberculosis with small bowel perforation: a case report.J Med Case Rep. 2021 Mar 31;15(1):144. doi: 10.1186/s13256-021-02752-2. J Med Case Rep. 2021. PMID: 33785067 Free PMC article.
-
MR and CT angiography in the diagnosis of vasculitides.BJR Open. 2023 Sep 25;5(1):20220020. doi: 10.1259/bjro.20220020. eCollection 2023. BJR Open. 2023. PMID: 37953869 Free PMC article. Review.
-
Ulcerative Colitis Prone to Delayed Diagnosis in a Nigerian Population: Case Series.Ann Med Health Sci Res. 2015 Jul-Aug;5(4):311-3. doi: 10.4103/2141-9248.160188. Ann Med Health Sci Res. 2015. PMID: 26229722 Free PMC article.
-
New CT-based diagnoses of torso cancer is low in the emergency department setting.Emerg Radiol. 2019 Dec;26(6):633-638. doi: 10.1007/s10140-019-01715-x. Epub 2019 Aug 20. Emerg Radiol. 2019. PMID: 31432349
-
Role of multidetector computed tomography in patients with acute infectious colitis.World J Clin Cases. 2022 Apr 26;10(12):3686-3697. doi: 10.12998/wjcc.v10.i12.3686. World J Clin Cases. 2022. PMID: 35647171 Free PMC article.
References
-
- Fernandes TC, Castro R, Pinto D, Oliveira MI, Carneiro A, Cunha R (2011) Bowel wall thickening – a complex subject made simple. Electronic Poster presented at 2011 ESGAR meeting doi:10.5444/esgar2011/EE-063#_blank
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
