

Preserved coronary flow reserve effectively excludes high-risk coronary artery disease on angiography
- PMID: 24408896
- PMCID: PMC3962818
- DOI: 10.2967/jnumed.113.121442
Preserved coronary flow reserve effectively excludes high-risk coronary artery disease on angiography
Abstract
Myocardial perfusion imaging has limited sensitivity for the detection of high-risk coronary artery disease (CAD). We tested the hypothesis that a normal coronary flow reserve (CFR) would be helpful for excluding the presence of high-risk CAD on angiography.
Methods: We studied 290 consecutive patients undergoing (82)Rb PET within 180 d of invasive coronary angiography. High-risk CAD on angiography was defined as 2-vessel disease (≥ 70% stenosis), including the proximal left anterior descending artery; 3-vessel disease; or left main CAD (≥ 50% stenosis). Patients with prior Q wave myocardial infarction, elevated troponin levels between studies, prior coronary artery bypass grafting, a left ventricular ejection fraction of less than 40%, or severe valvular heart disease were excluded.
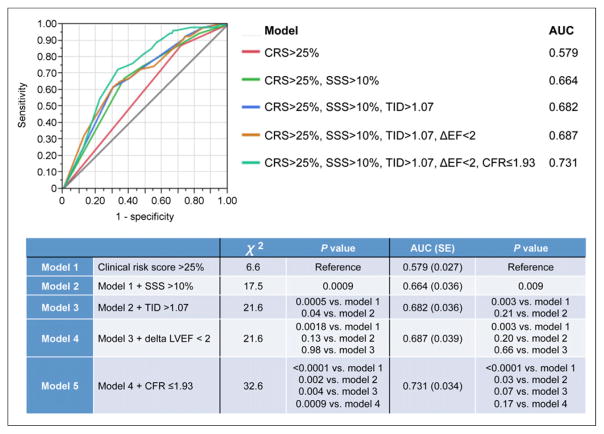
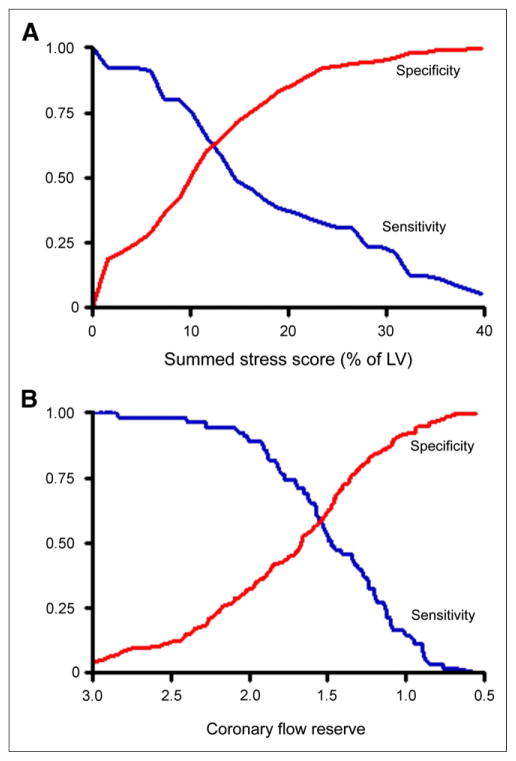
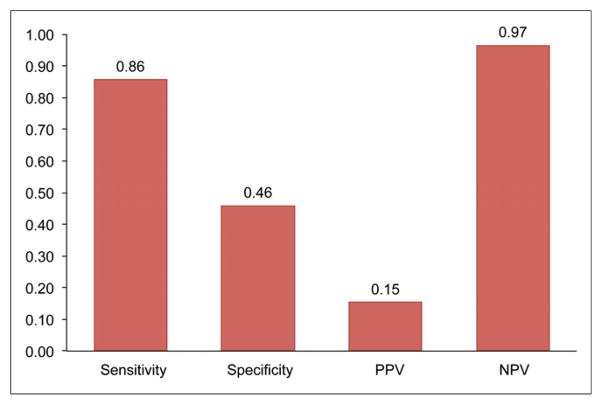
Results: Fifty-five patients (19%) had high-risk CAD on angiography. As expected, the trade-off between the sensitivity and the specificity of the CFR for identifying high-risk CAD varied substantially depending on the cutoff selected. In multivariable analysis, a binary CFR of less than or equal to 1.93 provided incremental diagnostic information for the identification of high-risk CAD beyond the model with the Duke clinical risk score (>25%), percentage of left ventricular ischemia (>10%), transient ischemic dilation index (>1.07), and change in the left ventricular ejection fraction during stress (<2) (P = 0.0009). In patients with normal or slightly to moderately abnormal results on perfusion scans (<10% of left ventricular mass) during stress (n = 136), a preserved CFR (>1.93) excluded high-risk CAD with a high sensitivity (86%) and a high negative predictive value (97%).
Conclusion: A normal CFR has a high negative predictive value for excluding high-risk CAD on angiography. Although an abnormal CFR increases the probability of significant obstructive CAD, it cannot reliably distinguish significant epicardial stenosis from nonobstructive, diffuse atherosclerosis or microvascular dysfunction.
Keywords: 82Rb PET; coronary artery disease; coronary flow reserve.
Figures

References
-
- Hendel RC, Berman DS, Di Carli MF, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. Circulation. 2009;119:e561–e587. - PubMed
-
- Shaw LJ, Hage FG, Berman DS, Hachamovitch R, Iskandrian A. Prognosis in the era of comparative effectiveness research: where is nuclear cardiology now and where should it be? J Nucl Cardiol. 2012;19:1026–1043. - PubMed
-
- Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107:2900–2907. - PubMed
-
- Fiechter M, Ghadri JR, Gebhard C, et al. Diagnostic value of 13N-ammonia myocardial perfusion PET: added value of myocardial flow reserve. J Nucl Med. 2012;53:1230–1234. - PubMed
-
- Ziadi MC, Dekemp RA, Williams K, et al. Does quantification of myocardial flow reserve using rubidium-82 positron emission tomography facilitate detection of multivessel coronary artery disease? J Nucl Cardiol. 2012;19:670–680. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous