

Refining pathological evaluation of neoadjuvant therapy for adenocarcinoma of the esophagus
- PMID: 24409055
- PMCID: PMC3882401
- DOI: 10.3748/wjg.v19.i48.9282
Refining pathological evaluation of neoadjuvant therapy for adenocarcinoma of the esophagus
Abstract
Aim: To assess tumour regression grade (TRG) and lymph node downstaging to help define patients who benefit from neoadjuvant chemotherapy.
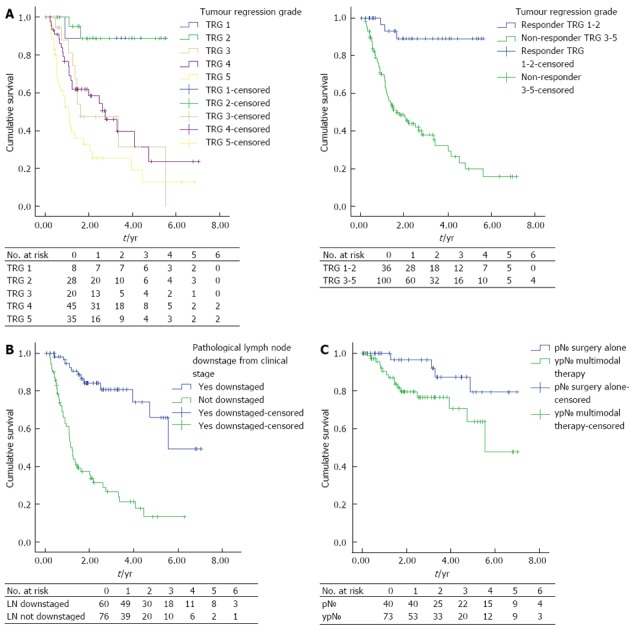
Methods: Two hundred and eighteen consecutive patients with adenocarcinoma of the esophagus or gastro-esophageal junction treated with surgery alone or neoadjuvant chemotherapy and surgery between 2005 and 2011 at a single institution were reviewed. Triplet neoadjuvant chemotherapy consisting of platinum, fluoropyrimidine and anthracycline was considered for operable patients (World Health Organization performance status ≤ 2) with clinical stage T2-4 N0-1. Response to neoadjuvant chemotherapy (NAC) was assessed using TRG, as described by Mandard et al. In addition lymph node downstaging was also assessed. Lymph node downstaging was defined by cN1 at diagnosis: assessed radiologically (computed tomography, positron emission tomography, endoscopic ultrasonography), then pathologically recorded as N0 after surgery; ypN0 if NAC given prior to surgery, or pN0 if surgery alone. Patients were followed up for 5 years post surgery. Recurrence was defined radiologically, with or without pathological confirmation. An association was examined between t TRG and lymph node downstaging with disease free survival (DFS) and a comprehensive range of clinicopathological characteristics.
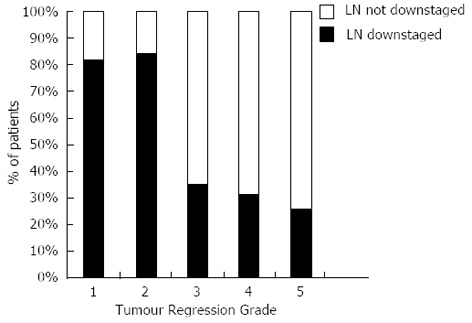
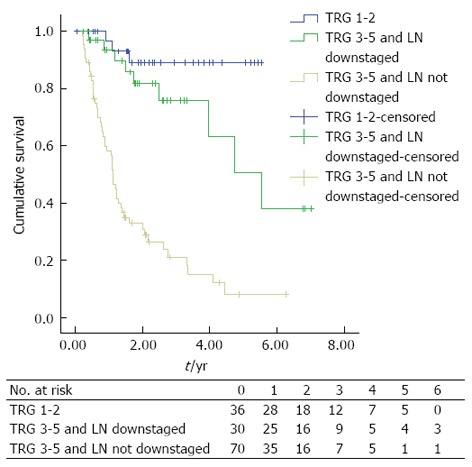
Results: Two hundred and eighteen patients underwent esophageal resection during the study interval with a mean follow up of 3 years (median follow up: 2.552, 95%CI: 2.022-3.081). There was a 1.8% (n = 4) inpatient mortality rate. One hundred and thirty-six (62.4%) patients received NAC, with 74.3% (n = 101) of patients demonstrating some signs of pathological tumour regression (TRG 1-4) and 5.9% (n = 8) having a complete pathological response. Forty four point one percent (n = 60) had downstaging of their nodal disease (cN1 to ypN0), compared to only 15.9% (n = 13) that underwent surgery alone (pre-operatively overstaged: cN1 to pN0), (P < 0.0001). Response to NAC was associated with significantly increased DFS (mean DFS; TRG 1-2: 5.1 years, 95%CI: 4.6-5.6 vs TRG 3-5: 2.8 years, 95%CI: 2.2-3.3, P < 0.0001). Nodal down-staging conferred a significant DFS advantage for those patients with a poor primary tumour response to NAC (median DFS; TRG 3-5 and nodal down-staging: 5.533 years, 95%CI: 3.558-7.531 vs TRG 3-5 and no nodal down-staging: 1.114 years, 95%CI: 0.961-1.267, P < 0.0001).
Conclusion: Response to NAC in the primary tumour and in the lymph nodes are both independently associated with improved DFS.
Keywords: Esophageal cancer; Gastro-esophageal cancer; Neoadjuvant; Regression.
Figures
References
-
- Allum WH, Blazeby JM, Griffin SM, Cunningham D, Jankowski JA, Wong R. Guidelines for the management of oesophageal and gastric cancer. Gut. 2011;60:1449–1472. - PubMed
-
- Langer R, Ott K, Feith M, Lordick F, Siewert JR, Becker K. Prognostic significance of histopathological tumor regression after neoadjuvant chemotherapy in esophageal adenocarcinomas. Mod Pathol. 2009;22:1555–1563. - PubMed
-
- Bollschweiler E, Hölscher AH, Metzger R, Besch S, Mönig SP, Baldus SE, Drebber U. Prognostic significance of a new grading system of lymph node morphology after neoadjuvant radiochemotherapy for esophageal cancer. Ann Thorac Surg. 2011;92:2020–2027. - PubMed
-
- Kelsen DP, Ginsberg R, Pajak TF, Sheahan DG, Gunderson L, Mortimer J, Estes N, Haller DG, Ajani J, Kocha W, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med. 1998;339:1979–1984. - PubMed
-
- Matsuyama J, Doki Y, Yasuda T, Miyata H, Fujiwara Y, Takiguchi S, Yamasaki M, Makari Y, Matsuura N, Mano M, et al. The effect of neoadjuvant chemotherapy on lymph node micrometastases in squamous cell carcinomas of the thoracic esophagus. Surgery. 2007;141:570–580. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
