

Endoscopic management of a rare granulation polyp in a colonic diverticulum
- PMID: 24409079
- PMCID: PMC3882425
- DOI: 10.3748/wjg.v19.i48.9481
Endoscopic management of a rare granulation polyp in a colonic diverticulum
Abstract
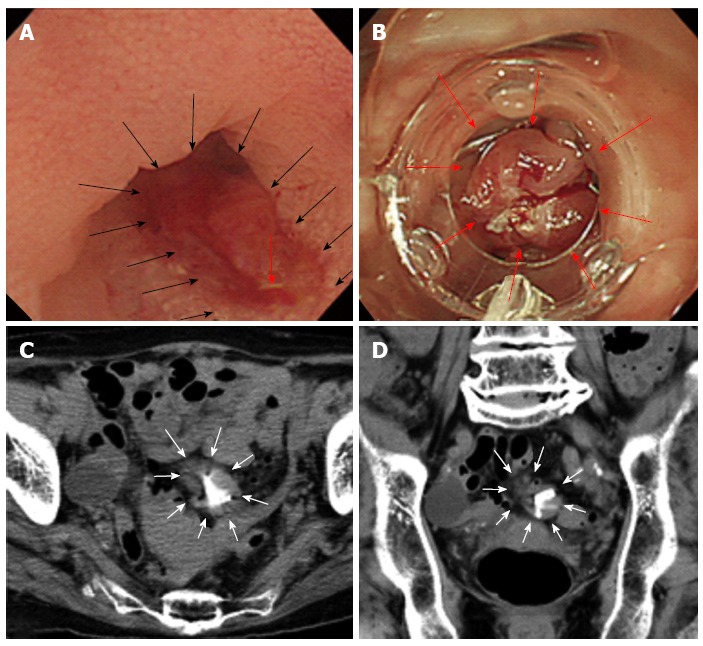
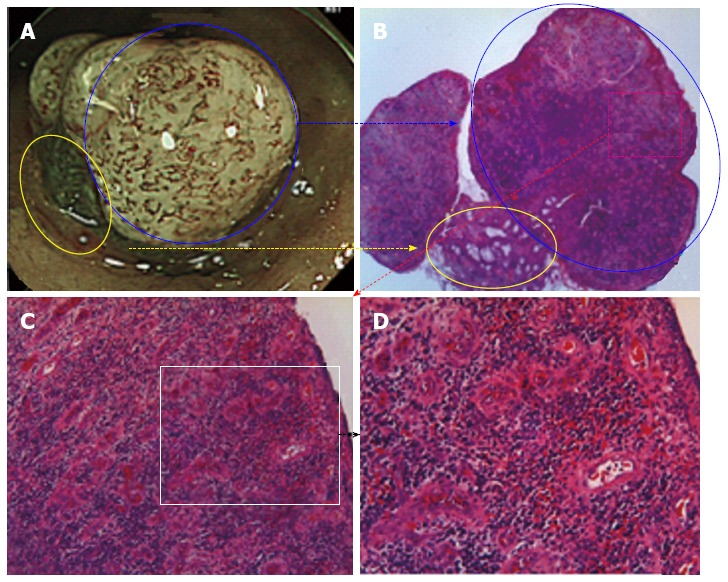
There are many case reports on colon diverticula that cause irritable bowel syndrome, constipation, bleeding, diverticulitis, stricture due to multiple recurrences of diverticulitis, and perforation. However, few articles have examined neoplasms that arise from a diverticulum, such as adenoma and adenocarcinoma, and there have been no reports of granulation polyps that arise from a colon diverticulum after recurrent diverticulitis. We observed a rare granulation polyp that arose from a diverticulum as a result of repeated episodes of local diverticulitis. Narrow band imaging magnified colonoscopy was very useful to diagnose the polyp as a granulation polyp because of the absence of a pit pattern on the surface of the polyp. We successfully resected the polyp using endoscopic mucosal resection. We inverted the diverticulum, and the resected stalk of the polyp was used to close the diverticulum with an over-the-scope clip. If a granulomatous polyp could arise from a diverticulum, differential diagnosis between a colon neoplasm and a granulomatous polyp would not only be difficult but also necessary for suitable endoscopic treatment.
Keywords: Diverticulitis; Endoscopy; Granulation polyp; Mucosal resection; Neoplasm; Recurrence.
Figures

References
-
- Maconi G, Barbara G, Bosetti C, Cuomo R, Annibale B. Treatment of diverticular disease of the colon and prevention of acute diverticulitis: a systematic review. Dis Colon Rectum. 2011;54:1326–1338. - PubMed
-
- Yoshida M, Kawabata K, Kutsumi H, Fujita T, Soga T, Nishimura K, Kawanami C, Kinoshita Y, Chiba T, Fujimoto S. Polypoid prolapsing mucosal folds associated with diverticular disease in the sigmoid colon: usefulness of colonoscopy and endoscopic ultrasonography for the diagnosis. Gastrointest Endosc. 1996;44:489–491. - PubMed
-
- Ishii N, Setoyama T, Deshpande GA, Omata F, Matsuda M, Suzuki S, Uemura M, Iizuka Y, Fukuda K, Suzuki K, et al. Endoscopic band ligation for colonic diverticular hemorrhage. Gastrointest Endosc. 2012;75:382–387. - PubMed
-
- Setoyama T, Ishii N, Fujita Y. Enodoscopic band ligation (EBL) is superior to endoscopic clipping for the treatment of colonic diverticular hemorrhage. Surg Endosc. 2011;25:3574–3578. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
