

Treatment of complex neurovascular lesions: an interdisciplinary angio suite approach
- PMID: 24409203
- PMCID: PMC3886381
- DOI: 10.1177/1756285613496861
Treatment of complex neurovascular lesions: an interdisciplinary angio suite approach
Abstract
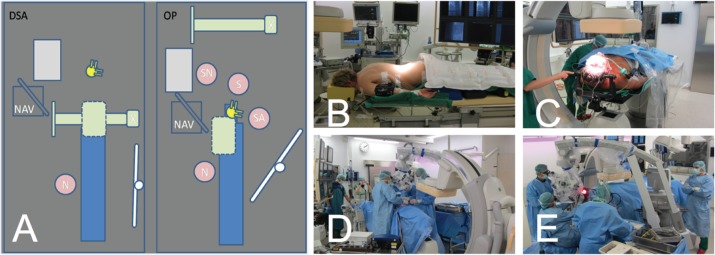
Objective: The objective of this study was to analyse our initial experience using an interdisciplinary angio suite approach to neurosurgical treatment of complex neurovascular lesions and expound technical feasibility and possible applications.
Subjects: Six out of 451 patients with cranial or spinal neurovascular lesions were surgically treated in the angio suite (biplane angiographic system) during a 28-month observation period. Clinical baseline data, radiological and intraoperative findings as well as clinical and radiological outcome were assessed.
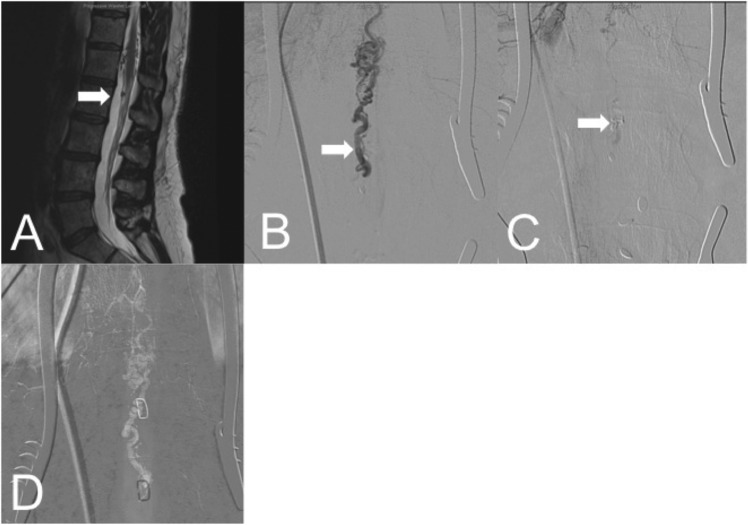
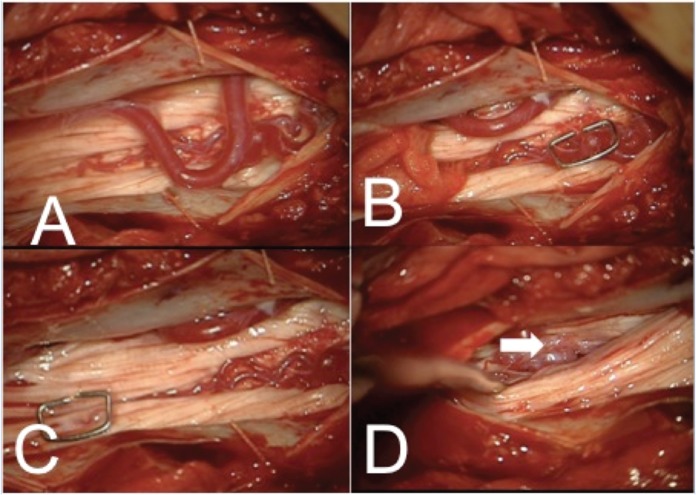
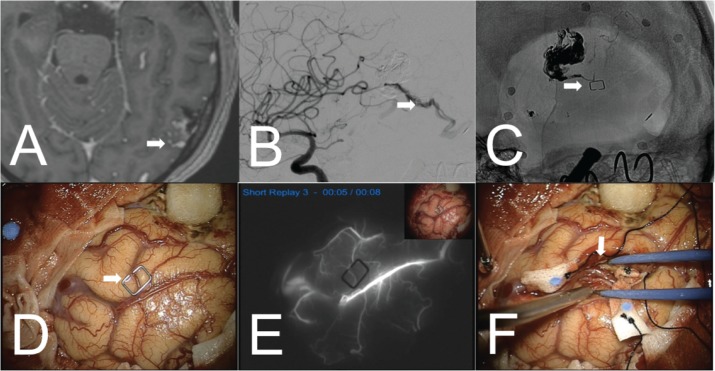
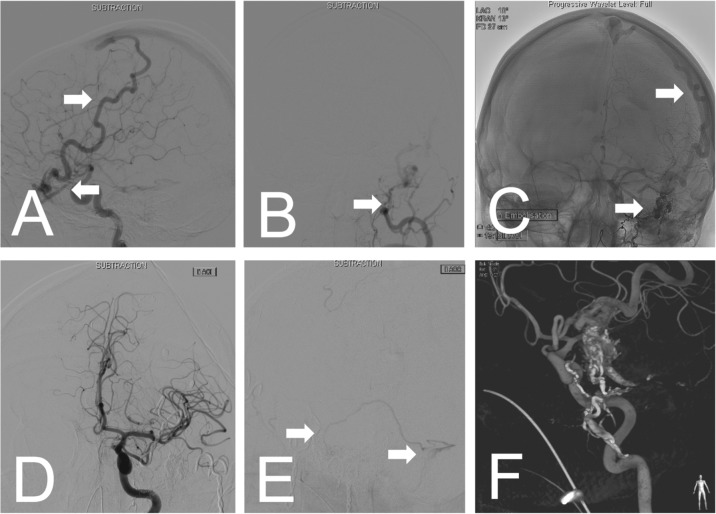
Results: A ventral spinal perimedullary arteriovenous malformation, a ventral spinal perimedullary fistula, two diffuse frontal dural arteriovenous fistulas, a multifocal temporal arteriovenous malformation and a partially embolized fronto-temporo-basal dural arteriovenous fistula were successfully treated with angiographically confirmed complete occlusion and unimpaired neurological condition of the patients at the 12-month follow up.
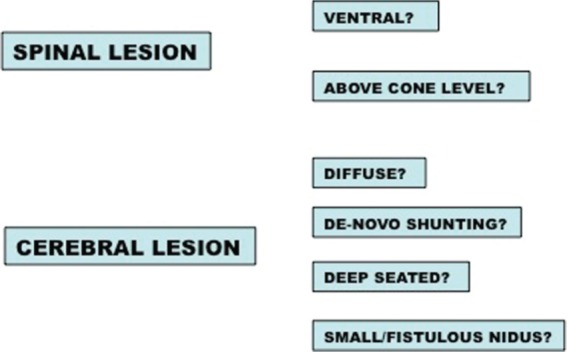
Conclusion: This study demonstrates the feasibility of this approach and points out possible indications, namely ventrally located spinal lesions and diffuse, deep seated cranial lesions.
Keywords: arteriovenous malformation; dural arteriovenous fistula; intraoperative angiography; neurovascular; surgical treatment.
Conflict of interest statement
Figures
References
-
- Barrow D., Boyer K., Joseph G. (1992) Intraoperative angiography in the management of neurovascular disorders. Neurosurgery 30: 153–159 - PubMed
-
- Benes L., Wakat J., Sure U., Bien S., Bertalanffy H. (2003) Intraoperative spinal digital subtraction angiography: technique and results. Neurosurgery 52: 603-609; discussion 608–609. - PubMed
-
- Chalouhi N., Theofanis T., Jabbour P., Dumont A., Gonzalez L., Starke R., et al. (2012) Safety and efficacy of intra-operative angiography in craniotomies for cerebral aneurysms and arteriovenous malformations: a review of 1089 cases. Neurosurgery 71(2): E550–E551 - PubMed
-
- Dehdashti A., Thines L., Da Costa L., terBrugge K., Willinsky R., Wallace M., et al. (2009) Intraoperative biplanar rotational angiography during neurovascular surgery. Technical note. J Neurosurg 111: 188–192 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
