

Tumor phenotype and breast density in distinct categories of interval cancer: results of population-based mammography screening in Spain
- PMID: 24410848
- PMCID: PMC3979164
- DOI: 10.1186/bcr3595
Tumor phenotype and breast density in distinct categories of interval cancer: results of population-based mammography screening in Spain
Abstract
Introduction: Interval cancers are tumors arising after a negative screening episode and before the next screening invitation. They can be classified into true interval cancers, false-negatives, minimal-sign cancers, and occult tumors based on mammographic findings in screening and diagnostic mammograms. This study aimed to describe tumor-related characteristics and the association of breast density and tumor phenotype within four interval cancer categories.
Methods: We included 2,245 invasive tumors (1,297 screening-detected and 948 interval cancers) diagnosed from 2000 to 2009 among 645,764 women aged 45 to 69 who underwent biennial screening in Spain. Interval cancers were classified by a semi-informed retrospective review into true interval cancers (n = 455), false-negatives (n = 224), minimal-sign (n = 166), and occult tumors (n = 103). Breast density was evaluated using Boyd's scale and was conflated into: <25%; 25 to 50%; 50 to 75%; >75%. Tumor-related information was obtained from cancer registries and clinical records. Tumor phenotype was defined as follows: luminal A: ER+/HER2- or PR+/HER2-; luminal B: ER+/HER2+ or PR+/HER2+; HER2: ER-/PR-/HER2+; triple-negative: ER-/PR-/HER2-. The association of tumor phenotype and breast density was assessed using a multinomial logistic regression model. Adjusted odds ratios (OR) and 95% confidence intervals (95% CI) were calculated. All statistical tests were two-sided.
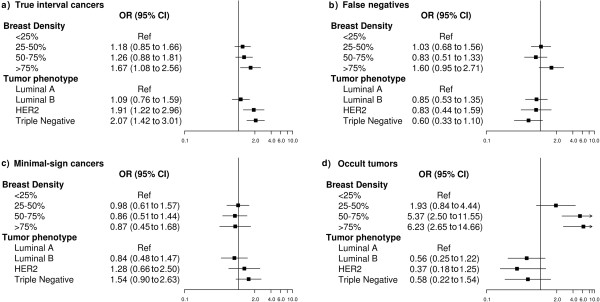
Results: Forty-eight percent of interval cancers were true interval cancers and 23.6% false-negatives. True interval cancers were associated with HER2 and triple-negative phenotypes (OR = 1.91 (95% CI:1.22-2.96), OR = 2.07 (95% CI:1.42-3.01), respectively) and extremely dense breasts (>75%) (OR = 1.67 (95% CI:1.08-2.56)). However, among true interval cancers a higher proportion of triple-negative tumors was observed in predominantly fatty breasts (<25%) than in denser breasts (28.7%, 21.4%, 11.3% and 14.3%, respectively; <0.001). False-negatives and occult tumors had similar phenotypic characteristics to screening-detected cancers, extreme breast density being strongly associated with occult tumors (OR = 6.23 (95% CI:2.65-14.66)). Minimal-sign cancers were biologically close to true interval cancers but showed no association with breast density.
Conclusions: Our findings revealed that both the distribution of tumor phenotype and breast density play specific and independent roles in each category of interval cancer. Further research is needed to understand the biological basis of the overrepresentation of triple-negative phenotype among predominantly fatty breasts in true interval cancers.
Figures
References
-
- Perry N, Broeders M, de Wolf C, Törnberg C, Holland R, von Karsa L. European guidelines for quality assurance in breast cancer screening and diagnosis. 4. Luxembourg: Office for Official Publications of the European Communities; 2006. - PubMed
-
- Domingo L, Sala M, Servitja S, Corominas JM, Ferrer F, Martinez J, Macia F, Quintana MJ, Albanell J, Castells X. Phenotypic characterization and risk factors for interval breast cancers in a population-based breast cancer screening program in Barcelona, Spain. Cancer Causes Control. 2010;21:1155–1164. doi: 10.1007/s10552-010-9541-6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
