

Myocarditis, hepatitis, and pancreatitis in a patient with coxsackievirus A4 infection: a case report
- PMID: 24410962
- PMCID: PMC3895747
- DOI: 10.1186/1743-422X-11-3
Myocarditis, hepatitis, and pancreatitis in a patient with coxsackievirus A4 infection: a case report
Abstract
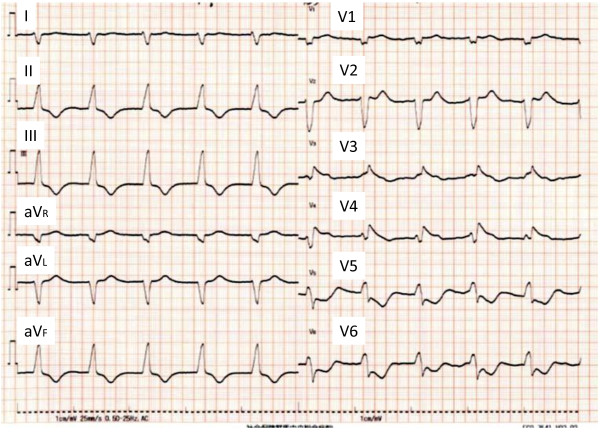
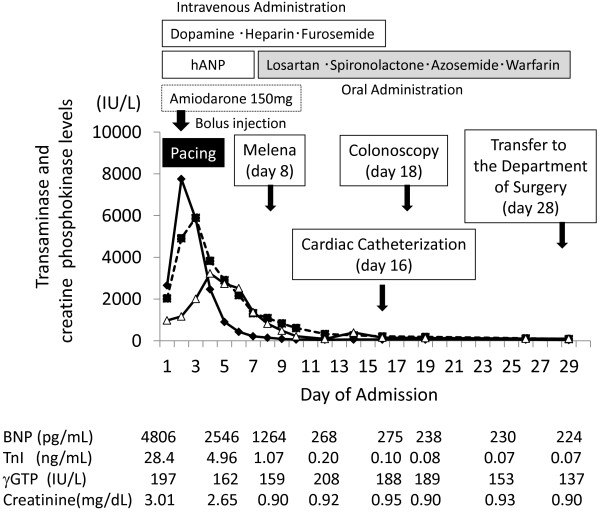
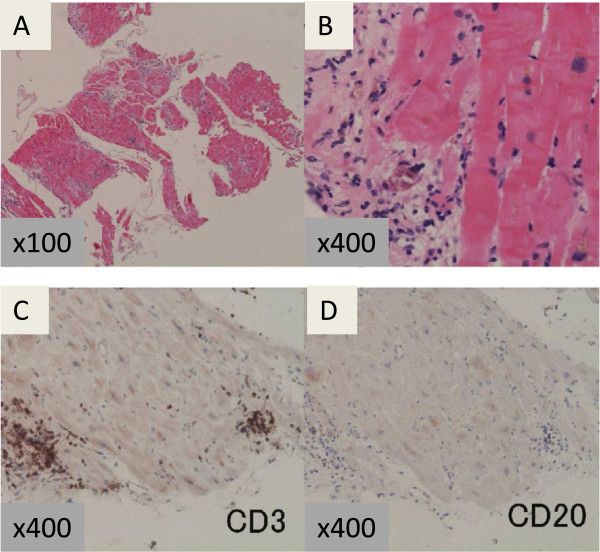
Viral myocarditis presents with various symptoms, including fatal arrhythmia and cardiogenic shock, and may develop chronic myocarditis and dilated cardiomyopathy in some patients. We report here a case of viral myocarditis with liver dysfunction and pancreatitis. A 63-year-old man was admitted to our hospital with dyspnea. The initial investigation showed pulmonary congestion, complete atrioventricular block, left ventricular dysfunction, elevated serum troponin I, and elevated liver enzyme levels. He developed pancreatitis five days after admission. Further investigation revealed a high antibody titer against coxsackievirus A4. The patient's left ventricular dysfunction, pancreatitis, and liver dysfunction had resolved by day 14, but his troponin I levels remained high, and an endomyocardial biopsy showed T-lymphocyte infiltration of the myocardium, confirming acute myocarditis. The patient underwent radical low anterior resection five weeks after admission for advanced rectal cancer found incidentally. His serum troponin I and plasma brain natriuretic peptide levels normalized six months after admission. He has now been followed-up for two years, and his left ventricular ejection fraction is stable.This is the first report of an adult with myocarditis and pancreatitis attributed to coxsackievirus A4. Combined myocarditis and pancreatitis arising from coxsackievirus infection is rare. This patient's clinical course suggests that changes in his immune response associated with his rectal cancer contributed to the amelioration of his viral myocarditis.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
