

The tumor radiobiology of SRS and SBRT: are more than the 5 Rs involved?
- PMID: 24411596
- PMCID: PMC3893711
- DOI: 10.1016/j.ijrobp.2013.07.022
The tumor radiobiology of SRS and SBRT: are more than the 5 Rs involved?
Abstract
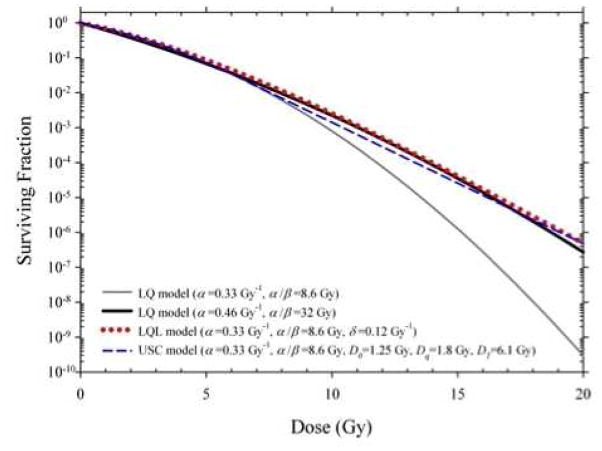
Stereotactic radiosurgery (SRS) and stereotactic body radiation therapy (SBRT), also known as stereotactic ablative radiation therapy (SABR), are rapidly becoming accepted practice for the radiation therapy of certain tumors. Typically, SRS and SBRT involve the delivery of 1 or a few large-dose fractions of 8 to 30 Gy per fraction: a major paradigm shift from radiation therapy practice over the past 90 years, when, with relatively large amounts of normal tissues receiving high doses, the goal was to maximize tumor response for an acceptable level of normal tissue injury. The development of SRS and SBRT have come about because of technologic advances in image guidance and treatment delivery techniques that enable the delivery of large doses to tumors with reduced margins and high gradients outside the target, thereby minimizing doses to surrounding normal tissues. Because the results obtained with SRS and SBRT have been impressive, they have raised the question whether classic radiobiological modeling, and the linear-quadratic (LQ) model, are appropriate for large doses per fraction. In addition to objections to the LQ model, the possibility of additional biological effects resulting from endothelial cell damage, enhanced tumor immunity, or both have been raised to account for the success of SRS and SBRT. In this review, we conclude that the available preclinical and clinical data do not support a need to change the LQ model or to invoke phenomena over and above the classic 5 Rs of radiobiology and radiation therapy, with the likely exception that for some tumors high doses of irradiation may produce enhanced antitumor immunity. Thus, we suggest that for most tumors, the standard radiobiology concepts of the 5 Rs are sufficient to explain the clinical data, and the excellent results obtained from clinical studies are the result of the much larger biologically effective doses that are delivered with SRS and SBRT.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none
Figures

Comment in
-
A hypothesis: indirect cell death in the radiosurgery era.Int J Radiat Oncol Biol Phys. 2015 Jan 1;91(1):11-3. doi: 10.1016/j.ijrobp.2014.08.355. Int J Radiat Oncol Biol Phys. 2015. PMID: 25835617 No abstract available.
References
-
- Withers HR. The four R’s of radiotherapy. In: Lett JTAH, editor. Advances in radiation biology. Vol. 5. New York: Academic Press; 1975. pp. 241–271.
-
- Steel GG, McMillan TJ, Peacock JH. The 5Rs of radiobiology. Int J Radiat Biol. 1989;56:1045–1048. - PubMed
-
- Sachs RK, Hahnfeld P, Brenner DJ. The link between low-LET dose-response relations and the underlying kinetics of damage production/repair/misrepair. International journal of radiation biology. 1997;72:351–374. - PubMed
-
- Carlson DJ, Stewart RD, Semenenko VA, et al. Combined use of Monte Carlo DNA damage simulations and deterministic repair models to examine putative mechanisms of cell killing. Radiat Res. 2008;169:447–459. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
