

Role of the carotid body chemoreceptors in baroreflex control of blood pressure during hypoglycaemia in humans
- PMID: 24414173
- PMCID: PMC4227537
- DOI: 10.1113/expphysiol.2013.076869
Role of the carotid body chemoreceptors in baroreflex control of blood pressure during hypoglycaemia in humans
Abstract
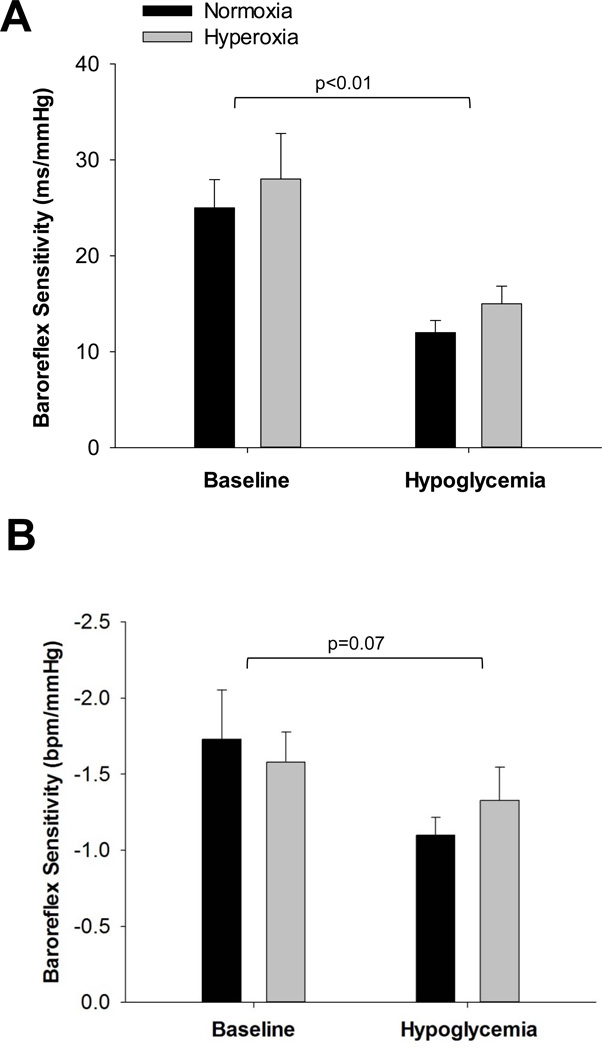
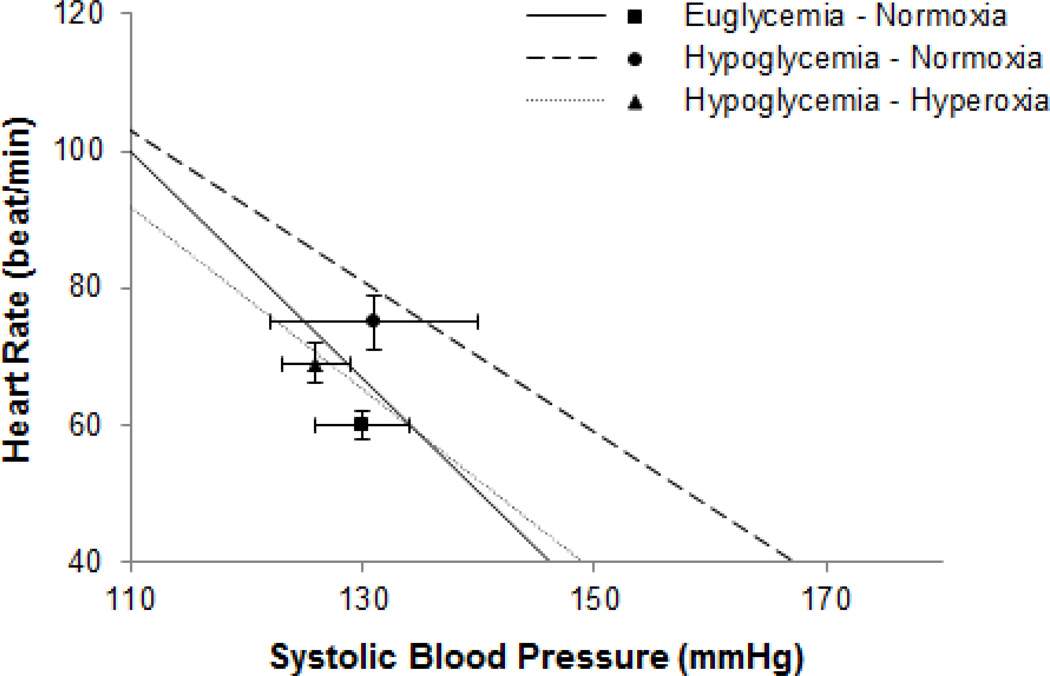
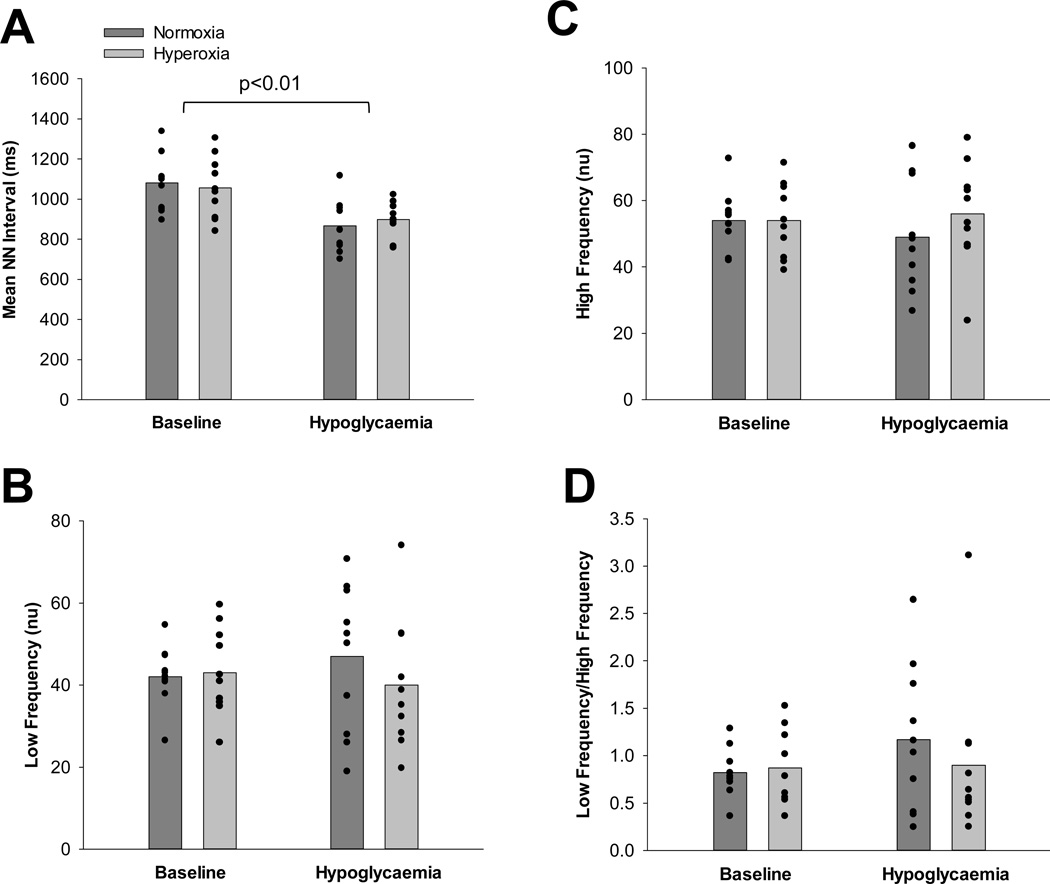
Activation of the carotid body chemoreceptors with hypoxia alters baroreceptor-mediated responses. We aimed to examine whether this relationship can be translated to other chemoreceptor stimuli (i.e. hypoglycaemia) by testing the following hypotheses: (i) activation of the carotid body chemoreceptors with hypoglycaemia would reduce spontaneous cardiac baroreflex sensitivity (sCBRS) in healthy humans; and (ii) desensitization of the carotid chemoreceptors with hyperoxia would restore sCBRS to baseline levels during hypoglycaemia. Ten young healthy adults completed two 180 min hyperinsulinaemic [2 mU (kg fat-free mass)(-1) min(-1)], hypoglycaemic (∼ 3.2 μmol ml(-1)) clamps, separated by at least 1 week and randomized to normoxia (arterial partial pressure of O2, 122 ± 10 mmHg) or hyperoxia (arterial partial pressure of O2, 424 ± 123 mmHg; to blunt activation of the carotid body glomus cells). Changes in heart rate, blood pressure, plasma catecholamines, heart rate variability (HRV) and sCBRS were assessed. During hypoglycaemia, HRV and sCBRS were reduced (P < 0.05) and the baroreflex working range was shifted to higher heart rates. When hyperoxia was superimposed on hypoglycaemia, there was a greater reduction in blood pressure and a blunted rise in heart rate when compared with normoxic conditions (P < 0.05); however, there was no detectable effect of hyperoxia on sCBRS or HRV during hypoglycaemia (P > 0.05). In summary, hypoglycaemia-mediated changes in HRV and sCBRS cannot be attributed exclusively to the carotid chemoreceptors; however, the chemoreceptors appear to play a role in resetting the baroreflex working range during hypoglycaemia.
Conflict of interest statement
Figures

References
-
- Alvarez-Buylla R, Alvarez-Buylla E, Mendoza H, Montero SA, Alvarez-Buylla A. Pituitary and adrenals are required for hyperglycemic reflex initiated by stimulation of CBR with cyanide. Am J Physiol. 1997;272:R392–R399. - PubMed
-
- Babu AR, Herdegen J, Fogelfeld L, Shott S, Mazzone T. Type 2 diabetes, glycemic control, and continuous positive airway pressure in obstructive sleep apnea. Arch Intern Med. 2005;165:447–452. - PubMed
-
- Basu R, Basu A, Johnson CM, Schwenk WF, Rizza RA. Insulin dose-response curves for stimulation of splanchnic glucose uptake and suppression of endogenous glucose production differ in nondiabetic humans and are abnormal in people with type 2 diabetes. Diabetes. 2004;53:2042–2050. - PubMed
-
- Biscoe TJ, Sampson SR. Stimulus response curves of single carotid body chemoreceptor afferent fibres. Nature. 1967;215:654–655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 NS032352/NS/NINDS NIH HHS/United States
- R01 DK029953/DK/NIDDK NIH HHS/United States
- NIH DK29953/DK/NIDDK NIH HHS/United States
- NIH 1 UL1RR024150/RR/NCRR NIH HHS/United States
- F32 DK084624/DK/NIDDK NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- NIH DK07352/DK/NIDDK NIH HHS/United States
- NIH NS32352/NS/NINDS NIH HHS/United States
- NIH F32 DK84624/DK/NIDDK NIH HHS/United States
- NIH T32 DK07352/DK/NIDDK NIH HHS/United States
- R01 DK090541/DK/NIDDK NIH HHS/United States
- N01 NS032352/NS/NINDS NIH HHS/United States
- R37 DK029953/DK/NIDDK NIH HHS/United States
- T32 DK007352/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous