

Prolonged lymphocytosis during ibrutinib therapy is associated with distinct molecular characteristics and does not indicate a suboptimal response to therapy
- PMID: 24415539
- PMCID: PMC3962160
- DOI: 10.1182/blood-2013-09-527853
Prolonged lymphocytosis during ibrutinib therapy is associated with distinct molecular characteristics and does not indicate a suboptimal response to therapy
Abstract
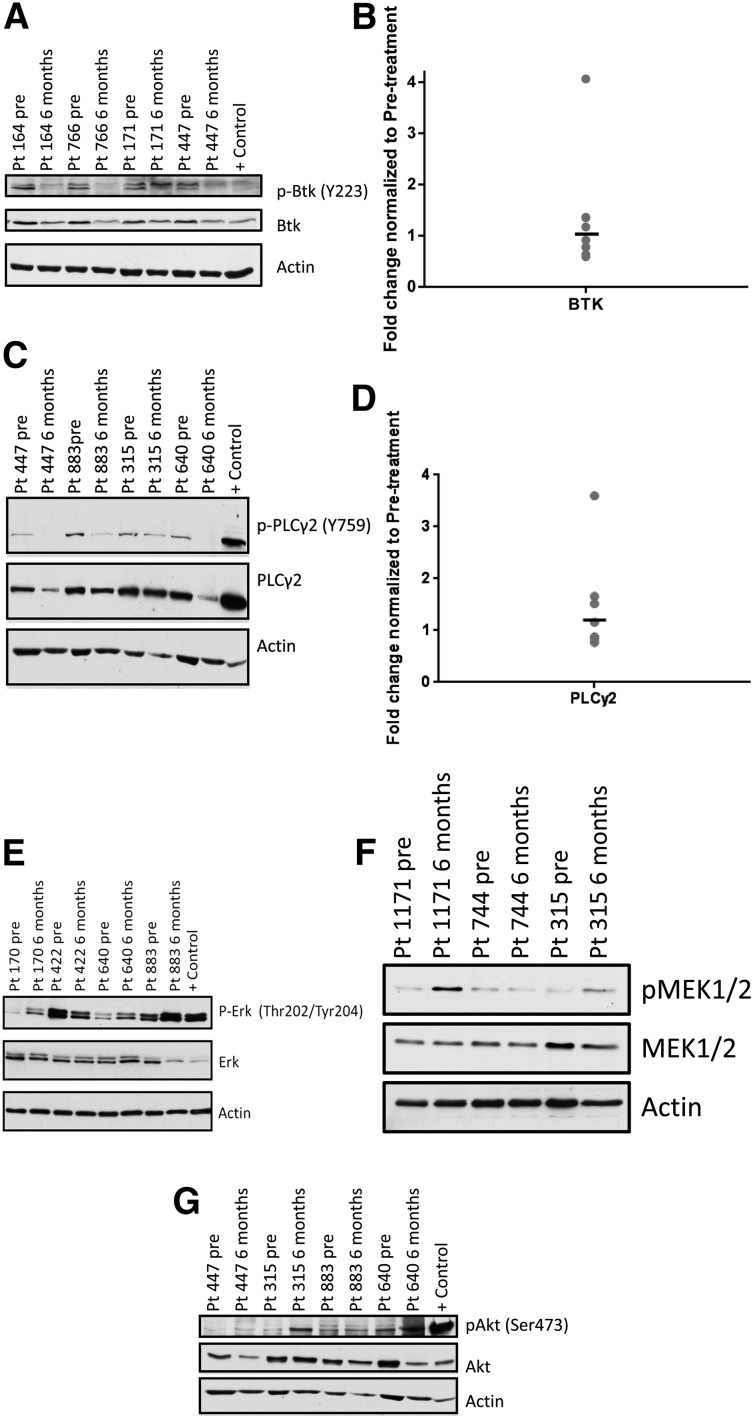
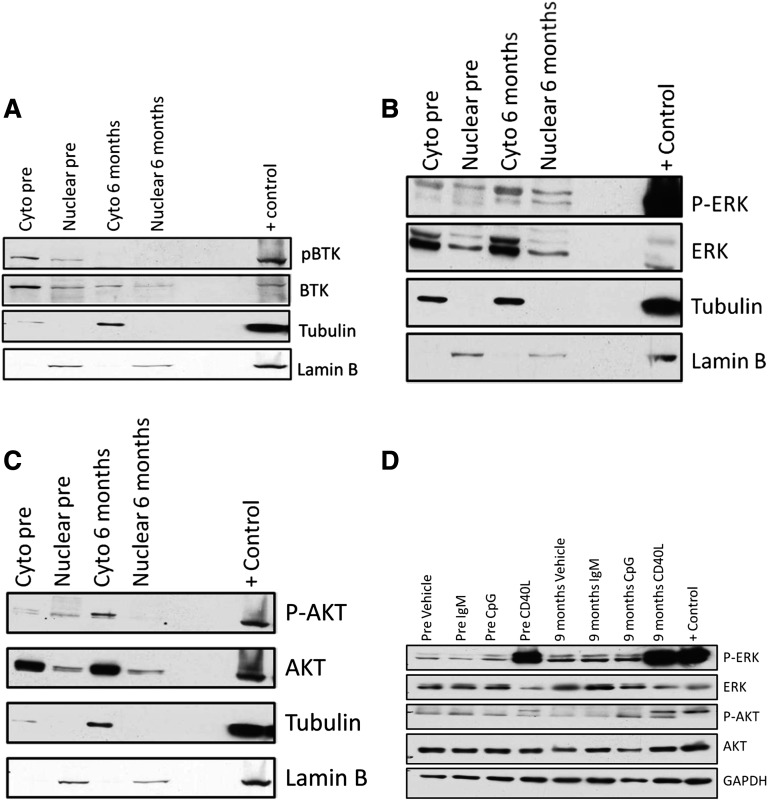
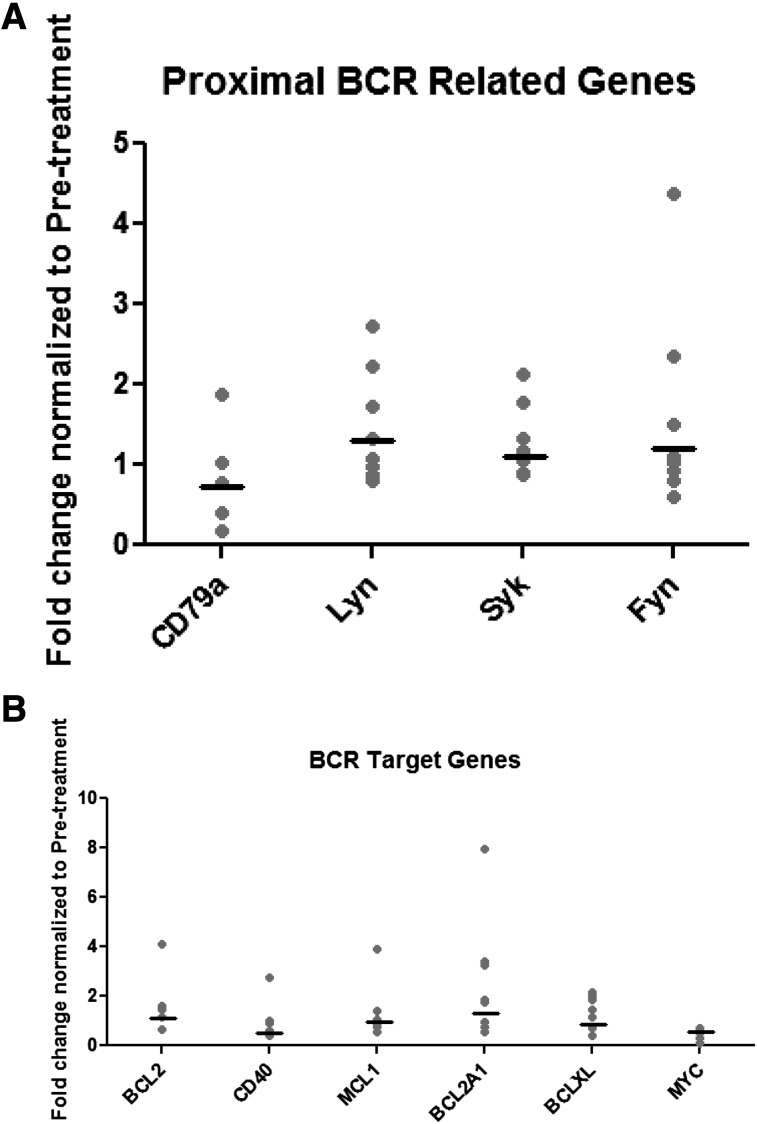
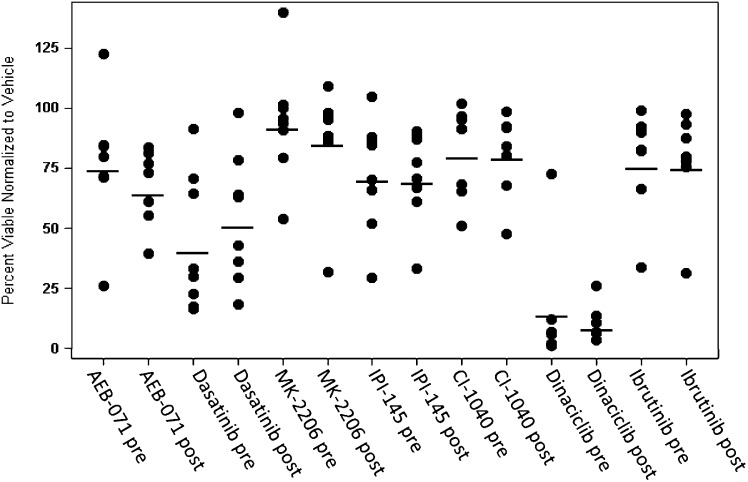
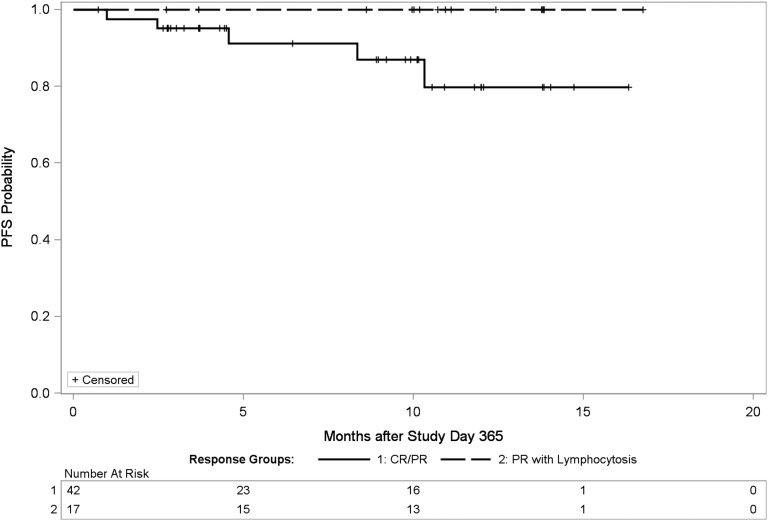
The Bruton's tyrosine kinase (BTK) inhibitor ibrutinib has outstanding activity in patients with chronic lymphocytic leukemia. Most patients experience lymphocytosis, representing lymphocyte egress from nodal compartments. This resolves within 8 months in the majority of patients, but a subgroup has lymphocytosis lasting >12 months. Here we report a detailed characterization of patients with persistent lymphocytosis during ibrutinib therapy. Signaling evaluation showed that while BTK is inhibited, downstream mediators of B-cell receptor (BCR) signaling are activated in persistent lymphocytes. These cells cannot be stimulated through the BCR and do not show evidence of target gene activation. Flow cytometry for κ and λ expression, IGHV sequencing, Zap-70 methylation, and targeted gene sequencing in these patients are identical at baseline and later time points, suggesting that persistent lymphocytes do not represent clonal evolution. In vitro treatment with targeted kinase inhibitors shows that they are not addicted to a single survival pathway. Finally, progression-free survival is not inferior for patients with prolonged lymphocytosis vs those with traditional responses. Thus, prolonged lymphocytosis is common following ibrutinib treatment, likely represents the persistence of a quiescent clone, and does not predict a subgroup of patients likely to relapse early.
Figures
Comment in
-
Lymphocytosis and ibrutinib treatment of CLL.Blood. 2014 Mar 20;123(12):1772-4. doi: 10.1182/blood-2014-01-549493. Blood. 2014. PMID: 24652958 No abstract available.
References
-
- Hallek M, Fischer K, Fingerle-Rowson G, et al. International Group of Investigators; German Chronic Lymphocytic Leukaemia Study Group. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–1174. - PubMed
-
- Byrd JC, Rai K, Peterson BL, et al. Addition of rituximab to fludarabine may prolong progression-free survival and overall survival in patients with previously untreated chronic lymphocytic leukemia: an updated retrospective comparative analysis of CALGB 9712 and CALGB 9011. Blood. 2005;105(1):49–53. - PubMed
-
- Morrison VA. Infectious complications of chronic lymphocytic leukaemia: pathogenesis, spectrum of infection, preventive approaches. Best Pract Res Clin Haematol. 2010;23(1):145–153. - PubMed
-
- Kath R, Blumenstengel K, Fricke HJ, Höffken K. Bendamustine monotherapy in advanced and refractory chronic lymphocytic leukemia. J Cancer Res Clin Oncol. 2001;127(1):48–54. - PubMed
-
- Dal Porto JM, Gauld SB, Merrell KT, Mills D, Pugh-Bernard AE, Cambier J. B cell antigen receptor signaling 101. Mol Immunol. 2004;41(6-7):599–613. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
