

The associations of uric acid, cardiovascular and all-cause mortality in peritoneal dialysis patients
- PMID: 24416142
- PMCID: PMC3885378
- DOI: 10.1371/journal.pone.0082342
The associations of uric acid, cardiovascular and all-cause mortality in peritoneal dialysis patients
Abstract
Aims: To investigate whether uric acid (UA) is an independent predictor of cardiovascular (CV) and all-cause mortality in peritoneal dialysis (PD) patients after controlling for recognized CV risk factors.
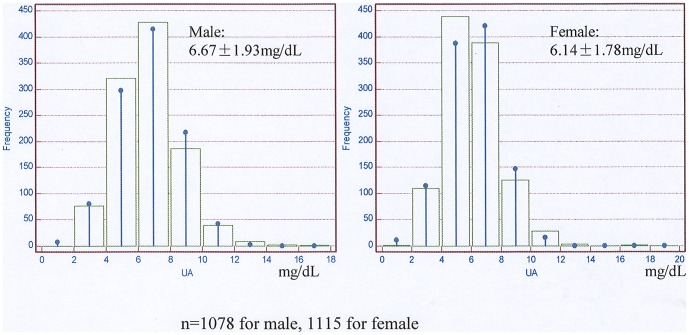
Methods: A total of 2264 patients on chronic PD were collected from seven centers affiliated with the Socioeconomic Status on the Outcome of Peritoneal Dialysis (SSOP) Study. All demographic and laboratory data were recorded at baseline. Multivariate Cox regression was used to calculate the hazard ratio (HR) of CV and all-cause mortality with adjustments for recognized traditional and uremia-related CV factors.
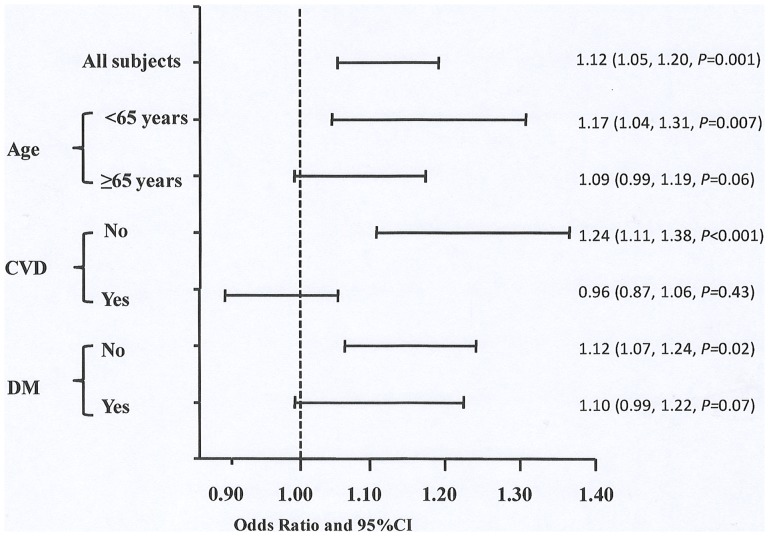
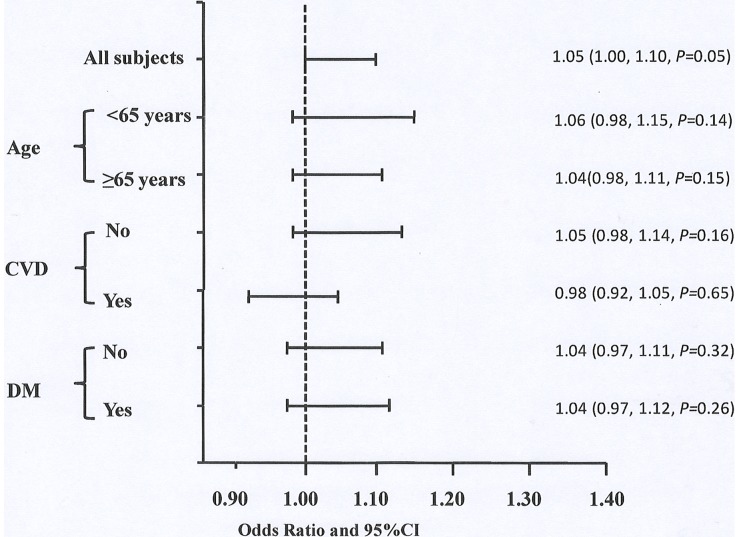
Results: There were no significant differences in baseline characteristics between patients with (n = 2193) and without (n = 71) UA measured. Each 1 mg/dL of increase in UA was associated with higher all-cause mortality with 1.05(1.00∼1.10) of HR and higher CV mortality with 1.12 (1.05∼1.20) of HR after adjusting for age, gender and center size. The highest gender-specific tertile of UA predicted higher all-cause mortality with 1.23(1.00∼1.52) of HR and higher CV mortality with 1.69 (1.21∼2.38) of HR after adjusting for age, gender and center size. The predictive value of UA was stronger in patients younger than 65 years without CV disease or diabetes at baseline. The prognostic value of UA as both continuous and categorical variable weakened or disappeared after further adjusted for uremia-related and traditional CV risk factors.
Conclusions: The prognostic value of UA in CV and all-cause mortality was weak in PD patients generally, which was confounded by uremia-related and traditional CV risk factors.
Conflict of interest statement
Figures
Similar articles
-
Relationship between serum uric acid, all-cause mortality and cardiovascular mortality in peritoneal dialysis patients: systematic review and meta-analysis of cohort studies.BMJ Open. 2021 Oct 18;11(10):e052274. doi: 10.1136/bmjopen-2021-052274. BMJ Open. 2021. PMID: 34663666 Free PMC article.
-
Uric acid to high-density lipoprotein cholesterol ratio predicts cardiovascular mortality in patients on peritoneal dialysis.Nutr Metab Cardiovasc Dis. 2021 Feb 8;31(2):561-569. doi: 10.1016/j.numecd.2020.10.005. Epub 2020 Oct 15. Nutr Metab Cardiovasc Dis. 2021. PMID: 33223397
-
Serum uric acid predicts cardiovascular mortality in male peritoneal dialysis patients with diabetes.Nutr Metab Cardiovasc Dis. 2016 Jan;26(1):20-6. doi: 10.1016/j.numecd.2015.10.011. Epub 2015 Nov 17. Nutr Metab Cardiovasc Dis. 2016. PMID: 26712272
-
Relationship between serum uric acid and all-cause and cardiovascular mortality in patients treated with peritoneal dialysis.Am J Kidney Dis. 2014 Aug;64(2):257-64. doi: 10.1053/j.ajkd.2013.08.027. Epub 2013 Oct 28. Am J Kidney Dis. 2014. PMID: 24176223
-
Risk factors for mortality in patients undergoing peritoneal dialysis: a systematic review and meta-analysis.Ren Fail. 2021 Dec;43(1):743-753. doi: 10.1080/0886022X.2021.1918558. Ren Fail. 2021. PMID: 33913381 Free PMC article.
Cited by
-
Relationship between serum uric acid, all-cause mortality and cardiovascular mortality in peritoneal dialysis patients: systematic review and meta-analysis of cohort studies.BMJ Open. 2021 Oct 18;11(10):e052274. doi: 10.1136/bmjopen-2021-052274. BMJ Open. 2021. PMID: 34663666 Free PMC article.
-
Association between mortality and serum uric acid levels in non-diabetes-related chronic kidney disease: An analysis of the National Health and Nutrition Examination Survey, USA, 1999-2010.Sci Rep. 2020 Oct 16;10(1):17585. doi: 10.1038/s41598-020-74747-w. Sci Rep. 2020. PMID: 33067501 Free PMC article.
-
How has peritoneal dialysis changed over the last 30 years: experience of the Verona dialysis center.BMC Nephrol. 2015 Apr 14;16:53. doi: 10.1186/s12882-015-0051-3. BMC Nephrol. 2015. PMID: 25885318 Free PMC article.
-
Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal Syndrome.Toxins (Basel). 2018 Sep 1;10(9):352. doi: 10.3390/toxins10090352. Toxins (Basel). 2018. PMID: 30200452 Free PMC article. Review.
-
Serum uric acid level and all-cause and cardiovascular mortality in peritoneal dialysis patients: A systematic review and dose-response meta-analysis of cohort studies.PLoS One. 2022 Feb 22;17(2):e0264340. doi: 10.1371/journal.pone.0264340. eCollection 2022. PLoS One. 2022. PMID: 35192651 Free PMC article.
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, et al. (2003) Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 42: 1050–1065. - PubMed
-
- Elsayed EF, Tighiouart H, Griffith J, Kurth T, Levey AS, et al. (2007) Cardiovascular disease and subsequent kidney disease. Arch Intern Med 167: 1130–1136. - PubMed
-
- USRDS Annual Data Report. Available: http://www.usrds.org/2011/view/v2_04.asp. Accessed 2013 Jun 3.
-
- Muntner P, He J, Astor BC, Folsom AR, Coresh J (2005) Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: results from the atherosclerosis risk in communities study. J Am Soc Nephrol 16: 529–538. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
