

Utility of T-cell interferon-γ release assays for diagnosing tuberculous serositis: a prospective study in Beijing, China
- PMID: 24416336
- PMCID: PMC3887014
- DOI: 10.1371/journal.pone.0085030
Utility of T-cell interferon-γ release assays for diagnosing tuberculous serositis: a prospective study in Beijing, China
Abstract
Background: Diagnosis of tuberculous serositis remains a challenge. The aim of this study was to evaluate the diagnostic efficiency of T-SPOT.TB on serous effusion mononuclear cells (SEMC) for diagnosing tuberculous serositis in a high TB burden area.
Methods: The present prospective study enrolled patients with suspected tuberculous serositis in a tertiary referral hospital in Beijing, China, to investigate the diagnostic sensitivity, specificity, predictive value (PV), and likelihood ratio(LR) of these tests. Clinical assessment, T-SPOT.TB on SEMC, and T-SPOT.TB on PBMC were performed. Test results were compared with the final confirmed diagnosis.
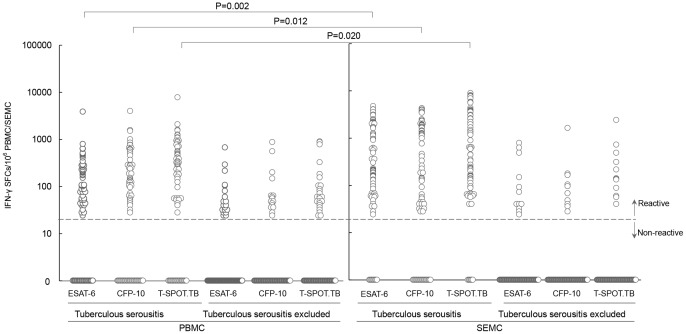
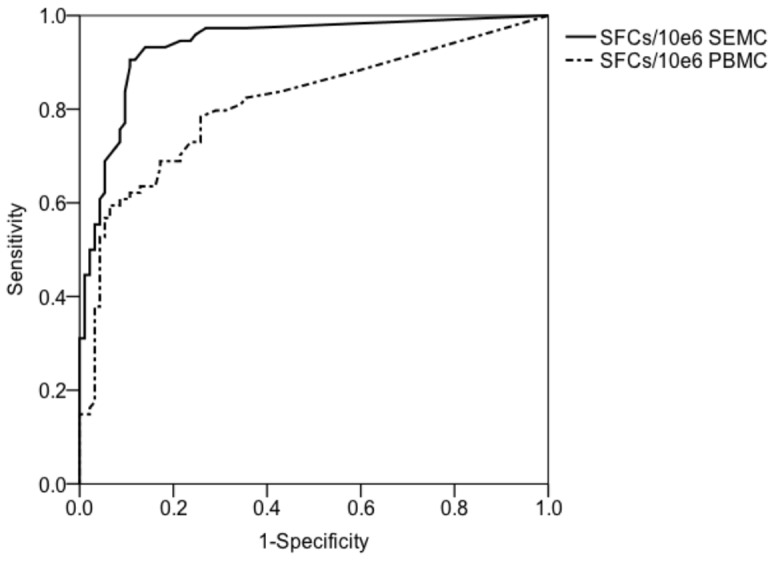
Results: Of the 187 participants, 74 (39.6%) were microbiologically or clinically diagnosed as tuberculous serositis and 93(49.7%) were ruled out. The remaining 20 (10.7%) patients were clinically indeterminate and excluded from the final analysis. Compared to that on PBMC, T-SPOT.TB on SEMC showed higher sensitivity (91.9%vs73.0%, P = 0.002), specificity (87.1%vs.73.1%, P = 0.017), PPV (85.0%vs.68.4%, P = 0.013), NPV (93.1%vs.77.3%, P = 0.003), LR+ (7.12vs.2.72) and LR- (0.09vs.0.37), respectively. The frequencies of spot forming cells (SFCs) for T-SPOT.TB on SEMC were 636 per million SEMC (IQR, 143-3443) in patients with tuberculous serositis, which were 4.6-fold (IQR, 1.3-14.3) higher than those of PBMC. By ROC curve analysis, a cut-off value of 56 SFCs per million SEMC for T-SPOT.TB on SEMC showed a sensitivity of 90.5% and specificity of 89.2% for the diagnosis of tuberculous serositis.
Conclusions: T-SPOT.TB on SEMC could be an accurate diagnostic method for tuberculous serositis in TB endemic settings. And 56 SFCs per million SEMC might be the optimal cut-off value to diagnose tuberculous serositis.
Conflict of interest statement
Figures
References
-
- Survey TGGotFNTE, Survey TOotFNTE (2012) The fifth national tuberculosis epidemiological survey in 2010. Chinese Journal of Antituberculosis 34.
-
- Jian-sheng H, Mei S, Ya-ling S (2000) Epidemiological Analysis of Extra-pulmonary Tuberculosis in Shanghai. CHINESE JOURNAL OF TUBERCULOSIS AND RESPIRATORY DISEASES 23 - PubMed
-
- Xi-rong W, Bao-ping X, An-xia J, Ying-Hui H, Qing-qin Y, et al.. (2012) The clinical epidemiological characteristics of pediatric tuberculosis in Beijing Children's Hospital from 2002 to 2010. CHINESE JOURNAL OF EVIDENCE BASED PEDIATRICS 07.
-
- Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR (2009) Epidemiology of extrapulmonary tuberculosis in the United States, 1993–2006. Clin Infect Dis 49: 1350–1357. - PubMed
-
- Sharma SK, Mohan A (2004) Extrapulmonary tuberculosis. Indian J Med Res 120: 316–353. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
