

Radiobiological comparison of two radiotherapy treatment techniques for high-risk prostate cancer
- PMID: 24416563
- PMCID: PMC3863222
- DOI: 10.1016/j.rpor.2012.12.006
Radiobiological comparison of two radiotherapy treatment techniques for high-risk prostate cancer
Abstract
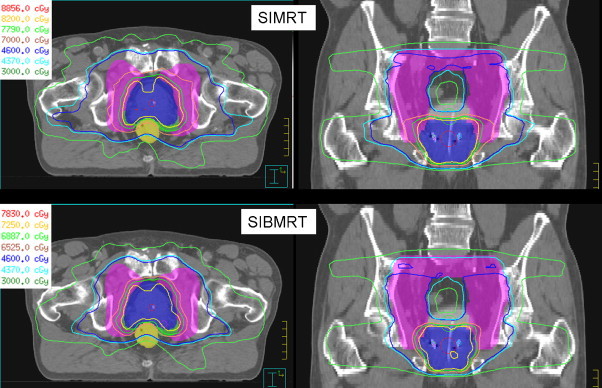
Background: To make a radiobiological comparison, for high risk prostate cancer (T3a, PSA > 20 ng/ml or Gleason > 7) of two radiotherapy treatment techniques. One technique consists of a treatment in three phases of the pelvic nodes, vesicles and prostate using a conventional fractionation scheme of 2 Gy/fraction (SIMRT). The other technique consists of a treatment in two phases that gives simultaneously different dose levels in each phase, 2 Gy/fraction, 2.25 Gy/fraction and 2.5 Gy/fraction to the pelvic nodes, vesicles and prostate, respectively (SIBIMRT).
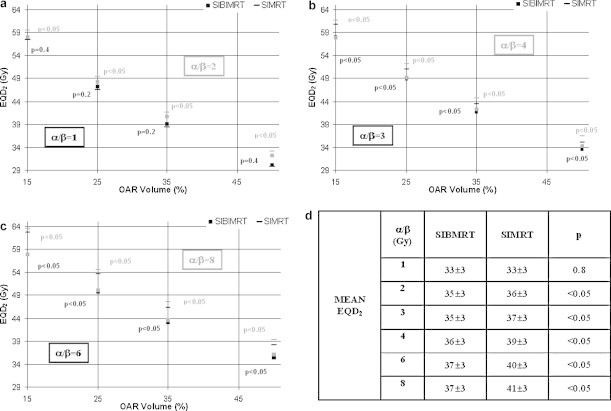
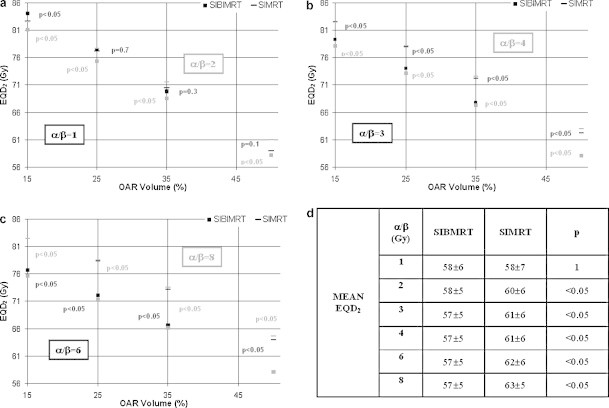
Materials and methods: The equivalent dose at fractionation of 2 Gy (EQD2), calculated using the linear quadratic model with α/β prostate = 1.5 Gy, was the same for both treatment strategies. For comparison the parameters employed were D95, mean dose and Tumour Control Probabilities for prostate PTV and D15, D25, D35, D50, mean dose and Normal Tissue Complication Probabilities for the rectum and bladder, with physical doses converted to EQD2. Parameters were obtained for α/β prostate = 1.5, 3 and 10 Gy and for α/β oar = 1, 2, 3, 4, 6 and 8.
Results: For prostate PTV, both treatment strategies are equivalent for α/β prostate = 1.5 Gy but for higher α/β prostate, EQD2 and TCP, decrease for the SIBIMRT technique. For the rectum and bladder when α/β oar ≤ 2 Gy, EQD2 and NTCP are lower for the SIMRT technique or equal in both techniques. For α/β oar ≥ 2-3 Gy, EQD2 and NTCP increase for the SIMRT treatment.
Conclusions: A comparison between two radiotherapy techniques is presented. The SIBIMRT technique reduces EQD2 and NTCP for α/β oar from 2 to 8 Gy.
Keywords: Equivalent dose at fractionation of 2 Gy (EQD2); NTCP; Prostate; Radiobiology; Simultaneous integrated boost.
Figures

References
-
- Wang J.Z., Guerrero M., Li X.A. How low is the a/b ratio for prostate cancer? Int J Radiat Oncol Biol Phys. 2003;55:194–203. - PubMed
-
- Fowler J., Chappell R., Ritter M. Is a/b for prostate tumors really low? Int J Radiat Oncol Biol Phys. 2001;50:1021–1031. - PubMed
-
- Dasu A. Is the alpha/beta value for prostate tumours low enough to be safely used in clinical trials? Clin Oncol (R Coll Radiol) 2007;19:289–301. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
