

Physicians' practices for diagnosing liver fibrosis in chronic liver diseases: a nationwide, Canadian survey
- PMID: 24416739
- PMCID: PMC4071896
- DOI: 10.1155/2014/675409
Physicians' practices for diagnosing liver fibrosis in chronic liver diseases: a nationwide, Canadian survey
Abstract
Objective: To determine practices among physicians in Canada for the assessment of liver fibrosis in patients with chronic liver diseases.
Methods: Hepatologists, gastroenterologists, infectious diseases specialists, members of the Canadian Gastroenterology Association and⁄or the Canadian HIV Trials Network who manage patients with liver diseases were invited to participate in a web-based, national survey.
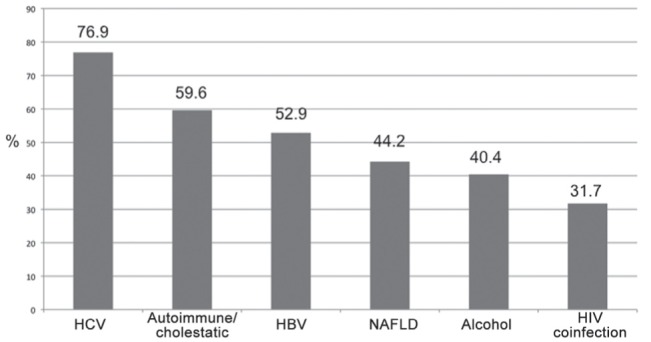
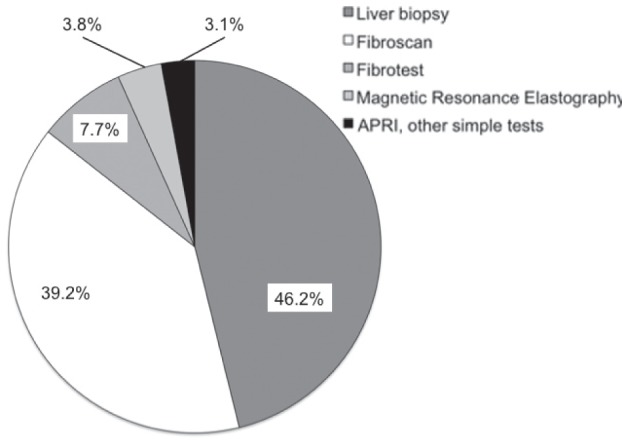
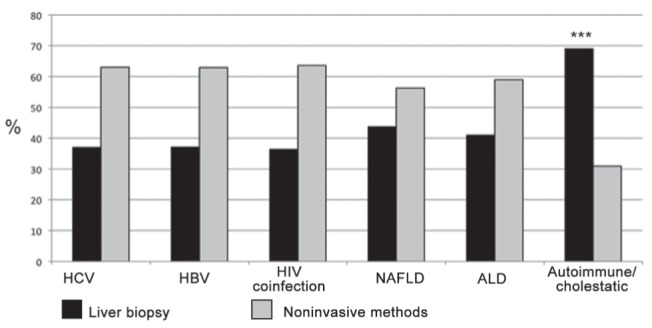
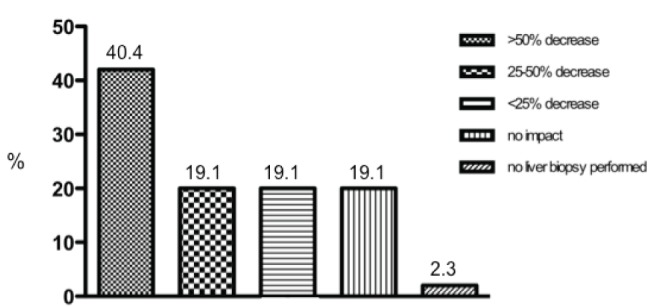
Results: Of the 237 physicians invited, 104 (43.9%) completed the survey. Routine assessment of liver fibrosis was requested by the surveyed physicians mostly for chronic hepatitis C (76.5%), followed by autoimmune⁄cholestatic liver disease (59.6%) and chronic hepatitis B (52.9%). Liver biopsy was the main diagnostic tool for 46.2% of the respondents, Fibroscan (Echosens, France) for 39.4% and Fibrotest (LabCorp, USA) for 7.7%. Etiology-specific differences were observed: noninvasive methods were mostly used for hepatitis C (63% versus 37% liver biopsy) and hepatitis B (62.9% versus 37.1% liver biopsy). For 42.7% of respondents, the use of noninvasive methods reduced the need for liver biopsy by >50%. Physicians' characteristics associated with higher use of noninvasive methods were older age and being based at a university hospital or in private practice versus community hospital. Physicians' main concerns regarding noninvasive fibrosis assessment methods were access⁄availability (42.3%), lack of guidelines for clinical use (26.9%) and cost⁄lack of reimbursement (14.4%).
Conclusions: Physicians who manage patients with chronic liver diseases in Canada require routine assessment of liver fibrosis stage. Although biopsy remains the primary diagnostic tool for almost one-half of respondents, noninvasive methods, particularly Fibroscan, have significantly reduced the need for liver biopsy in Canada. Limitations in access to and availability of the noninvasive methods represent a significant barrier. Finally, there is a need for clinical guidelines and a better reimbursement policy to implement noninvasive tools to assess liver fibrosis.
OBJECTIF :: Déterminer les pratiques des médecins du Canada en matière d’évaluation de la fibrose hépatique chez des patients atteints d’une maladie hépatique chronique.
MÉTHODOLOGIE :: Les hépatologistes, les gastroentérologues, les infectiologues, les membres de l’Association canadienne de gastroentérologie et ceux du Réseau pour les essais VIH qui prenaient en charge des patients ayant une maladie hépatique ont été invités à participer à un sondage virtuel national.
RÉSULTATS :: Sur les 237 médecins invités, 104 (43,9 %) ont rempli le sondage. Les médecins demandaient une évaluation systématique de la fibrose hépatique surtout en cas d’hépatite C chronique (76,5 %), de maladie hépatique auto-immune ou de maladie cholestatique du foie (59,6 %) et d’hépatite B chronique (52,9 %). La biopsie hépatique était le principal outil diagnostique pour 46,2 % des répondants, le Fibroscan (Echosens, France), pour 39,4 % d’entre eux, et le Fibrotest (LabCorp, États-Unis), pour 7,7 % d’entre eux. Les chercheurs ont observé des différences propres à l’étiologie : les méthodes non effractives étaient surtout utilisées en cas d’hépatite C (63 % par rapport à 37 % de biopsie hépatique) et d’hépatite B (62,9 % par rapport à 37,1 % de biopsie hépatique). Chez 42,7 % des répondants, le recours à une méthode non effractive réduisait de plus de 50 % la nécessité de biopsie hépatique. Les caractéristiques des médecins associées à une plus forte utilisation de méthodes non effractives étaient le fait d’être plus âgés et de travailler dans un hôpital universitaire ou en pratique privée plutôt que dans un hôpital général. Les principales inquiétudes des médecins à l’égard de l’évaluation non effractive de la fibrose étaient l’accès ou la disponibilité (42,3 %), l’absence de directives cliniques (26,9 %) et le coût ou l’absence de remboursement (14,4 %).
CONCLUSIONS :: Les médecins qui prennent en charge les patients ayant une maladie hépatique chronique au Canada demandent une évaluation systématique du stade de fibrose hépatique. Même si la biopsie demeure le principal outil diagnostique pour près de la moitié des répondants, les méthodes non effractives, notamment le Fibroscan, ont considérablement réduit la nécessité d’utiliser la biopsie hépatique au Canada. Les limites d’accès et de disponibilité des méthodes non effractives représentent un obstacle important. Enfin, il faudrait produire des directives cliniques et prévoir une meilleure politique de remboursement pour qu’on puisse adopter les outils non effractifs dans l’évaluation de la fibrose hépatique.
Figures
Comment in
-
Out with the old and in with the new: hepatic fibrosis assessment in Canada.Can J Gastroenterol Hepatol. 2014 Jan;28(1):20. doi: 10.1155/2014/496196. Can J Gastroenterol Hepatol. 2014. PMID: 24416737 Free PMC article. No abstract available.
References
-
- Fleming KM, Aithal GP, Solaymani-Dodaran M, Card TR, West J. Incidence and prevalence of cirrhosis in the United Kingdom, 1992–2001: A general population-based study. J Hepatol. 2008;49:732–8. - PubMed
-
- Kim WR, Brown RS, Jr, Terrault NA, El-Serag H. Burden of liver disease in the United States: Summary of a workshop. Hepatology. 2002;36:227–42. - PubMed
-
- Sanabria AJ, Dion R, Lucar E, Soto JC. Evolution of the determinants of chronic liver disease in Quebec. Chronic Dis Inj Can. 2013;33:137–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
