

A novel molecular microbiologic technique for the rapid diagnosis of microbial invasion of the amniotic cavity and intra-amniotic infection in preterm labor with intact membranes
- PMID: 24417618
- PMCID: PMC3954440
- DOI: 10.1111/aji.12189
A novel molecular microbiologic technique for the rapid diagnosis of microbial invasion of the amniotic cavity and intra-amniotic infection in preterm labor with intact membranes
Abstract
Problem: The diagnosis of microbial invasion of the amniotic cavity (MIAC) has been traditionally performed using traditional cultivation techniques, which require growth of microorganisms in the laboratory. Shortcomings of culture methods include the time required (days) for identification of microorganisms, and that many microbes involved in the genesis of human diseases are difficult to culture. A novel technique combines broad-range real-time polymerase chain reaction with electrospray ionization time-of-flight mass spectrometry (PCR/ESI-MS) to identify and quantify genomic material from bacteria and viruses.
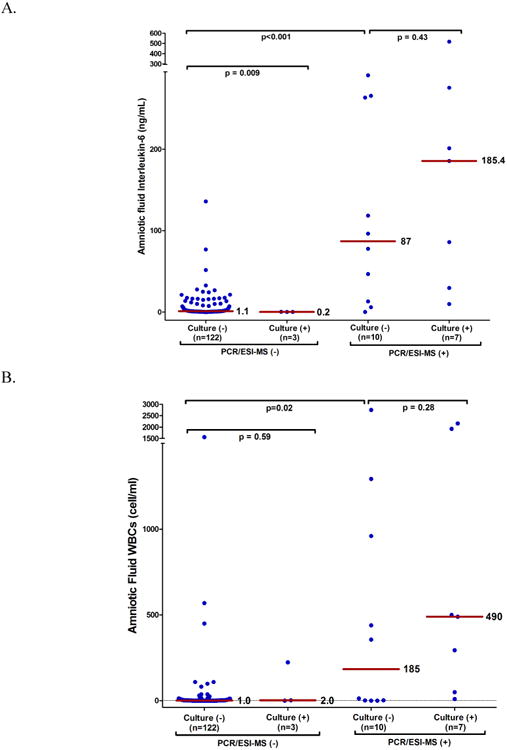
Method of study: AF samples obtained by transabdominal amniocentesis from 142 women with preterm labor and intact membranes (PTL) were analyzed using cultivation techniques (aerobic, anaerobic, and genital mycoplasmas) as well as PCR/ESI-MS. The prevalence and relative magnitude of intra-amniotic inflammation [AF interleukin 6 (IL-6) concentration ≥ 2.6 ng/mL], acute histologic chorioamnionitis, spontaneous preterm delivery, and perinatal mortality were examined.
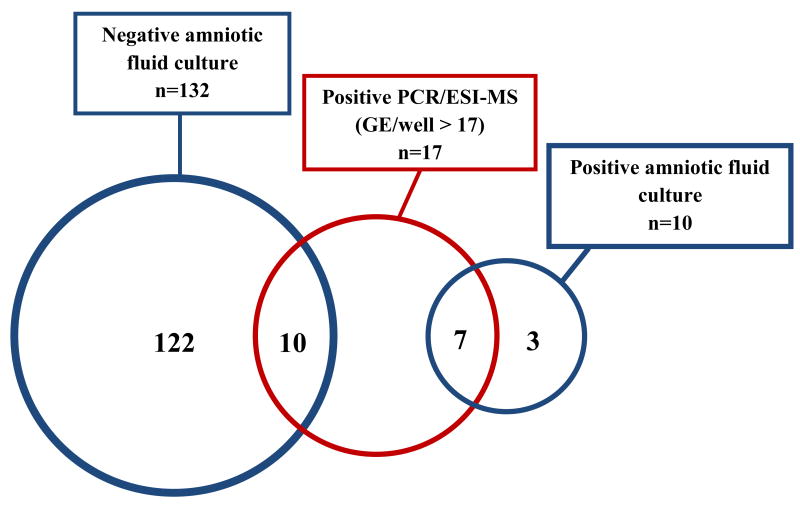
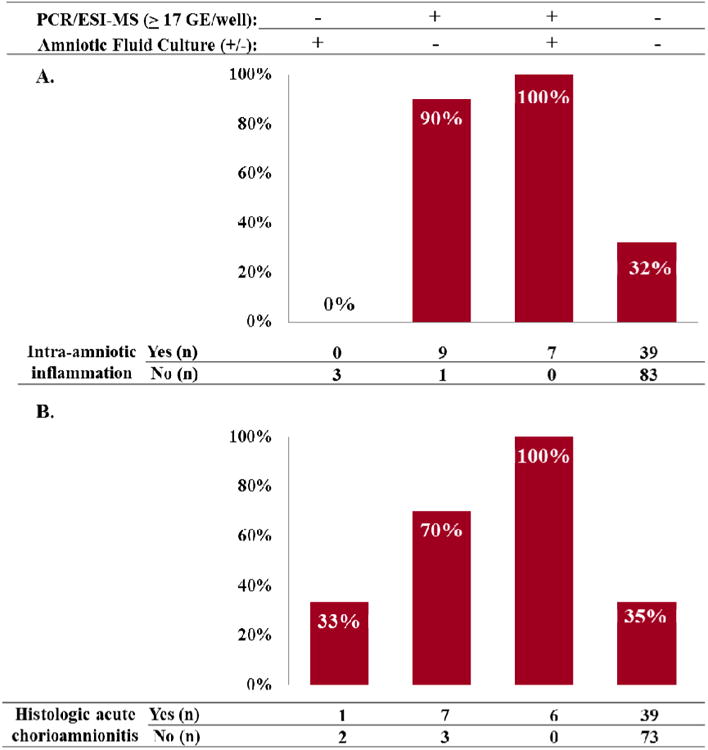
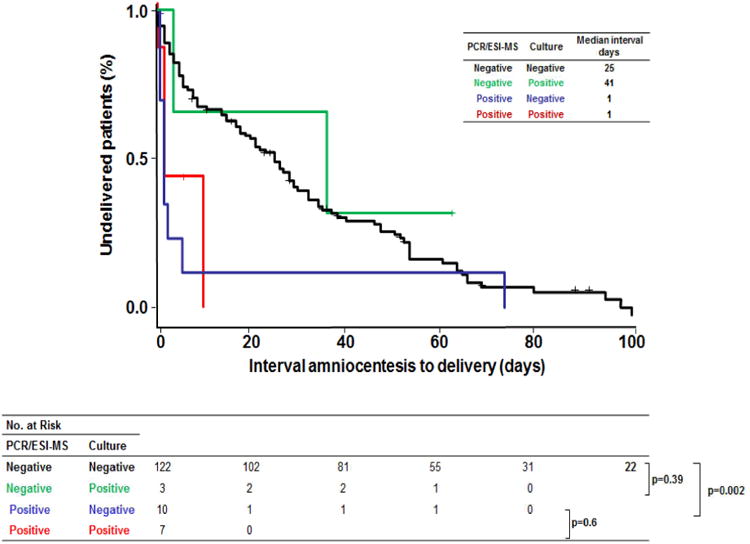
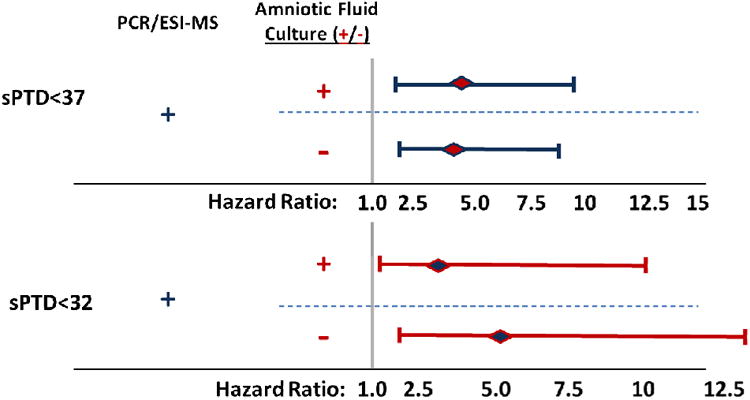
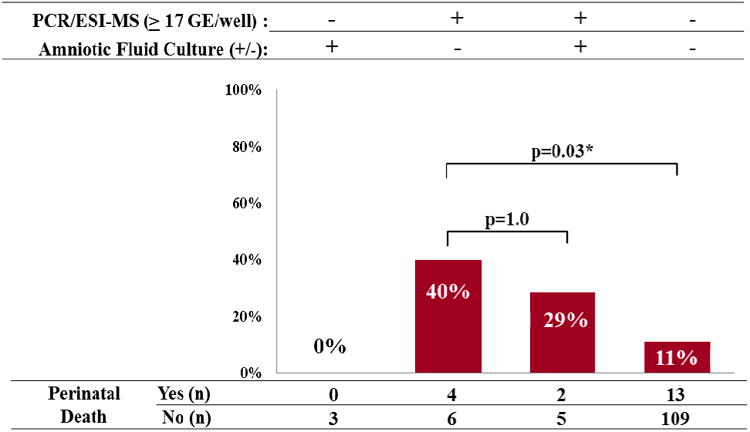
Results: (i) The prevalence of MIAC in patients with PTL was 7% using standard cultivation techniques and 12% using PCR/ESI-MS; (ii) seven of ten patients with positive AF culture also had positive PCR/ESI-MS [≥17 genome equivalents per PCR reaction well (GE/well)]; (iii) patients with positive PCR/ESI-MS (≥17 GE/well) and negative AF cultures had significantly higher rates of intra-amniotic inflammation and acute histologic chorioamnionitis, a shorter interval to delivery [median (interquartile range-IQR)], and offspring at higher risk of perinatal mortality, than women with both tests negative [90% (9/10) versus 32% (39/122) OR: 5.6; 95% CI: 1.4-22; (P < 0.001); 70% (7/10) versus 35% (39/112); (P = 0.04); 1 (IQR: <1-2) days versus 25 (IQR: 5-51) days; (P = 0.002), respectively]; (iv) there were no significant differences in these outcomes between patients with positive PCR/ESI-MS (≥17 GE/well) who had negative AF cultures and those with positive AF cultures; and (v) PCR/ESI-MS detected genomic material from viruses in two patients (1.4%).
Conclusion: (i) Rapid diagnosis of intra-amniotic infection is possible using PCR/ESI-MS; (ii) the combined use of biomarkers of inflammation and PCR/ESI-MS allows for the identification of specific bacteria and viruses in women with preterm labor and intra-amniotic infection; and (iii) this approach may allow for administration of timely and specific interventions to reduce morbidity attributed to infection-induced preterm birth.
Keywords: Broad-range real-time polymerase chain reaction, electrospray ionization mass spectrometry; inflammation; preterm delivery; time-of-flight.
Published 2014. This article is a U.S. Government work and is in the public domain in the USA.
Figures
References
-
- World Health Organization. WHO Library Cataloguing-in-Publication. World Health Organization; 2012. Born too soon: the global action report in preterm birth.
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L, Lawn JE. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–2172. - PubMed
-
- Dimes Mo., editor. March of dimes: Premature Birth. 2009.
-
- Muglia LJ, Katz M. The enigma of spontaneous preterm birth. N Engl J Med. 2010;362:529–535. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
