

Differential effect of genetic burden on disease phenotypes in Crohn's disease and ulcerative colitis: analysis of a North American cohort
- PMID: 24419484
- PMCID: PMC4225079
- DOI: 10.1038/ajg.2013.464
Differential effect of genetic burden on disease phenotypes in Crohn's disease and ulcerative colitis: analysis of a North American cohort
Abstract
Objectives: Crohn's disease (CD) and ulcerative colitis (UC) are chronic immunologically mediated diseases with a progressive relapsing remitting course. There is considerable heterogeneity in disease course and accurate prediction of natural history has been challenging. The phenotypic implication of increasing genetic predisposition to CD or UC is unknown.
Methods: The data source for our study was a prospective cohort of CD and UC patients recruited from a tertiary referral center. All patients underwent genotyping on the Illumina Immunochip. A genetic risk score (GRS) incorporating strength of association (log odds ratio) and allele dose for each of the 163 inflammatory bowel disease (IBD) risk loci was calculated and phenotypic associations examined across GRS quartiles.
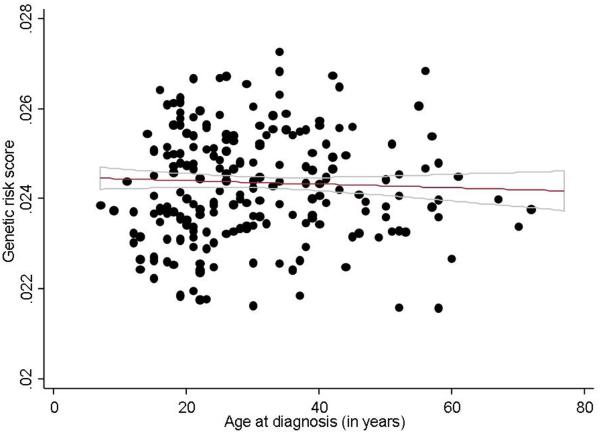
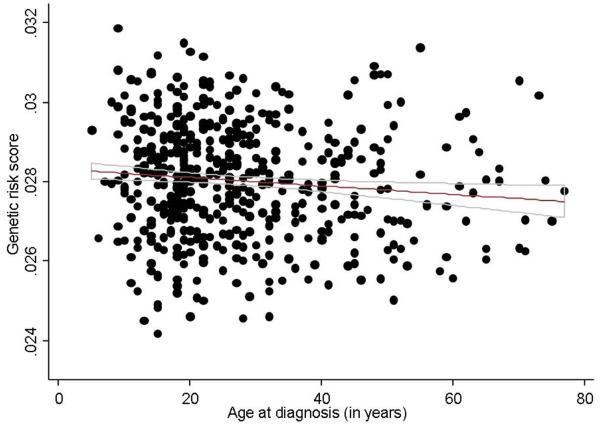
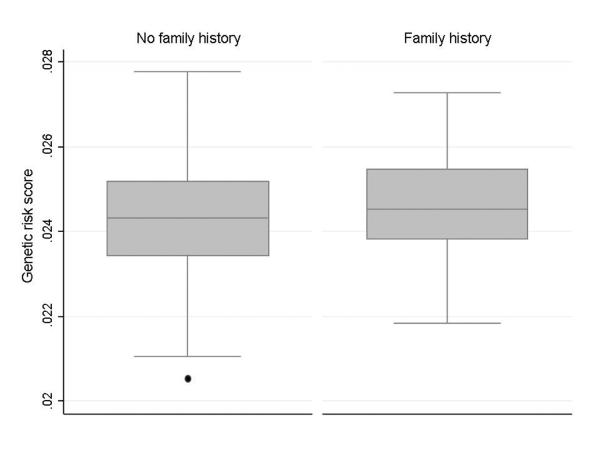
Results: Our study cohort included 1,105 patients (697 CD, 408 UC). Increasing genetic burden was associated with earlier age of diagnosis of CD (Ptrend=0.008). Patients in the highest GRS quartile were likely to develop disease 5 years earlier than those in the lowest quartile. Increasing genetic burden was also associated with ileal involvement in CD (Ptrend <0.0001). The effect of genetic burden was independent of the NOD2 locus and was stronger among those with no NOD2 variants, and in never smokers. UC patients with an involved first-degree relative had a higher genetic burden, but GRS was not associated with disease phenotype in UC.
Conclusions: Increasing genetic burden is associated with early age of diagnosis in CD, but not UC. The expanded panel of IBD risk loci explains only a fraction of variance of disease phenotype, suggesting limited clinical utility of genetics in predicting natural history.
Figures
References
-
- Loftus EV., Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental influences. Gastroenterology. 2004;126:1504–17. - PubMed
-
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54. e42; quiz e30. - PubMed
-
- Van Assche G, Lewis JD, Lichtenstein GR, Loftus EV, Ouyang Q, Panes J, Siegel CA, Sandborn WJ, Travis SP, Colombel JF. The London position statement of the World Congress of Gastroenterology on Biological Therapy for IBD with the European Crohn's and Colitis Organisation: safety. Am J Gastroenterol. 106:1594–602. quiz 1593, 1603. - PubMed
-
- D'Haens G, Baert F, van Assche G, Caenepeel P, Vergauwe P, Tuynman H, De Vos M, van Deventer S, Stitt L, Donner A, Vermeire S, Van de Mierop FJ, Coche JC, van der Woude J, Ochsenkuhn T, van Bodegraven AA, Van Hootegem PP, Lambrecht GL, Mana F, Rutgeerts P, Feagan BG, Hommes D. Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn's disease: an open randomised trial. Lancet. 2008;371:660–7. - PubMed
-
- Colombel JF, Sandborn WJ, Reinisch W, Mantzaris GJ, Kornbluth A, Rachmilewitz D, Lichtiger S, D'Haens G, Diamond RH, Broussard DL, Tang KL, van der Woude CJ, Rutgeerts P. Infliximab, azathioprine, or combination therapy for Crohn's disease. N Engl J Med. 2010;362:1383–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
