

Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States
- PMID: 24419737
- PMCID: PMC3959706
- DOI: 10.1161/JAHA.113.000590
Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States
Abstract
Background: Limited information is available on the contemporary and potentially changing trends in the incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction (STEMI).
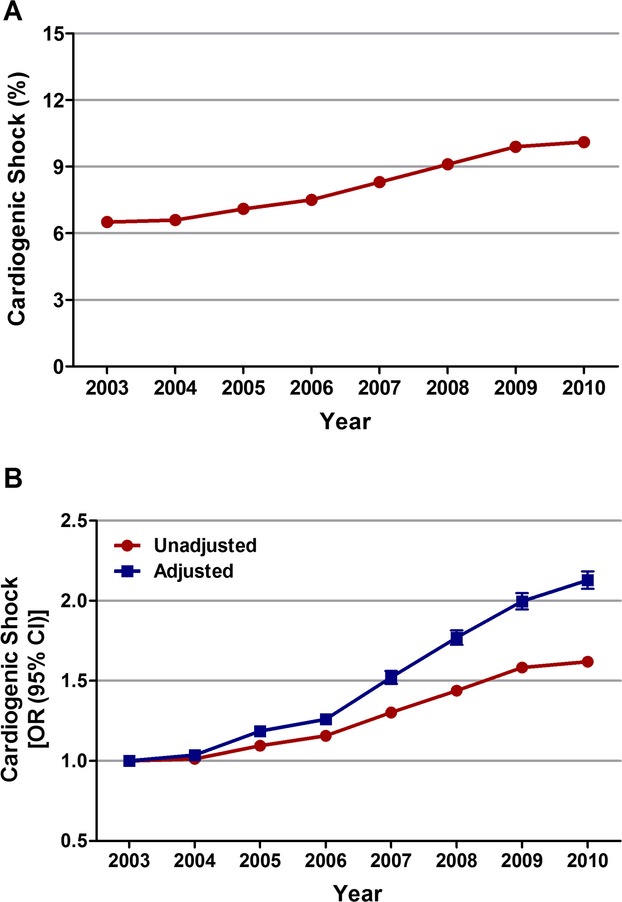
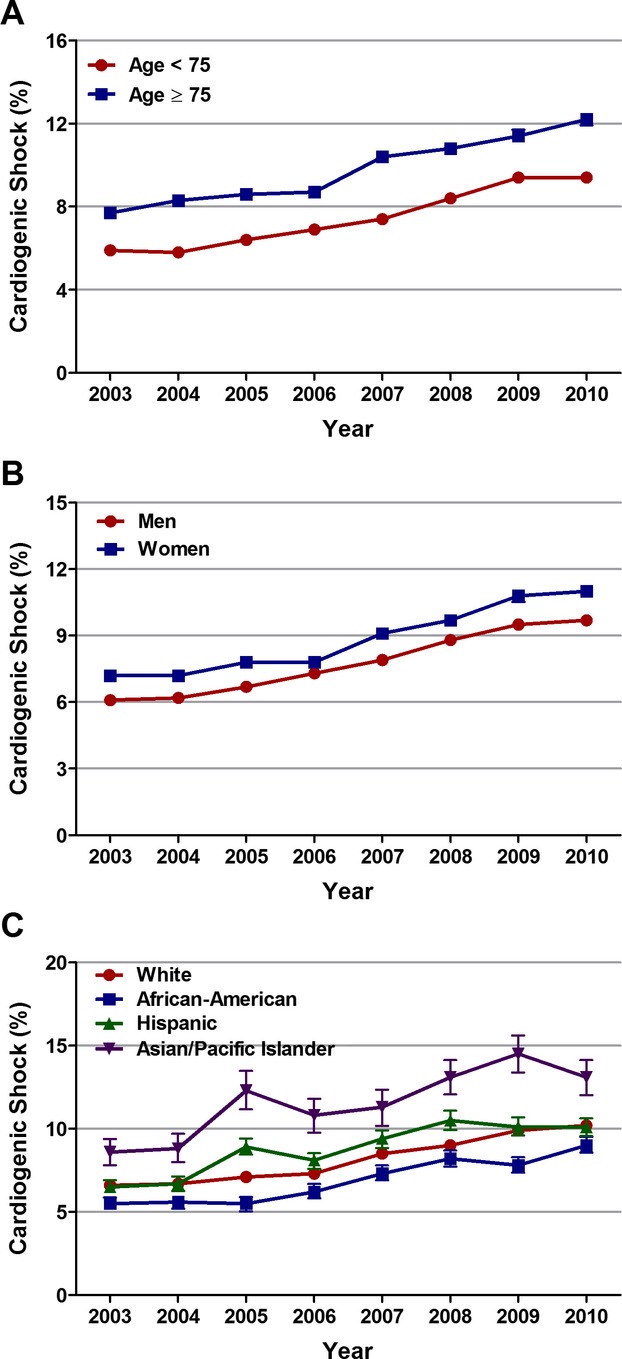
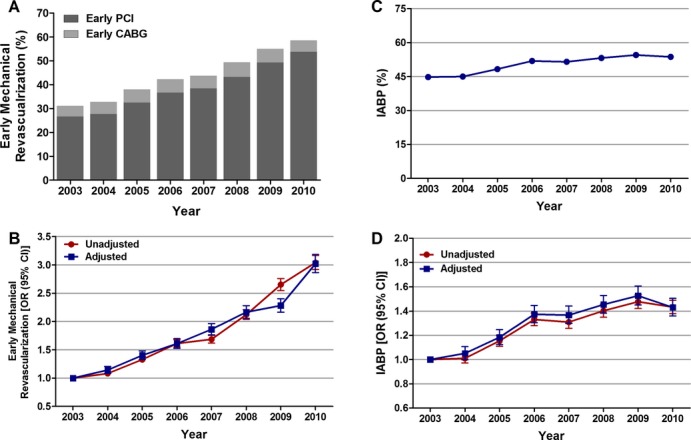
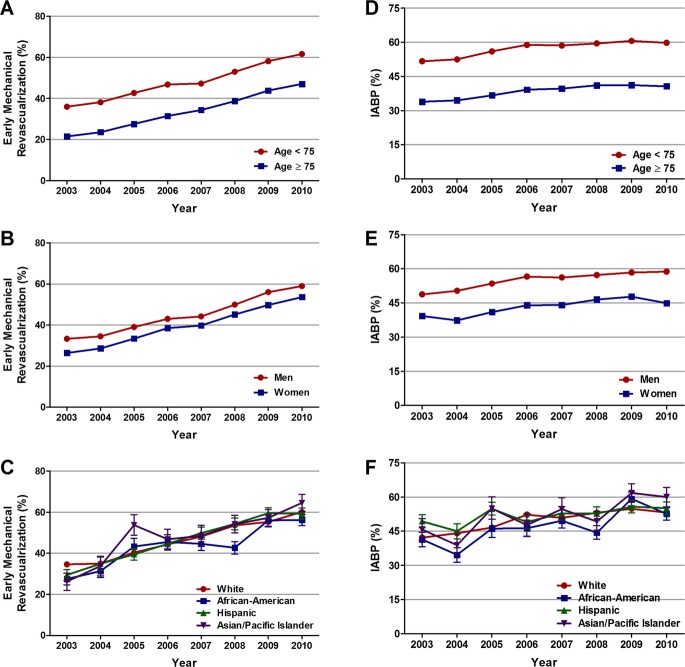
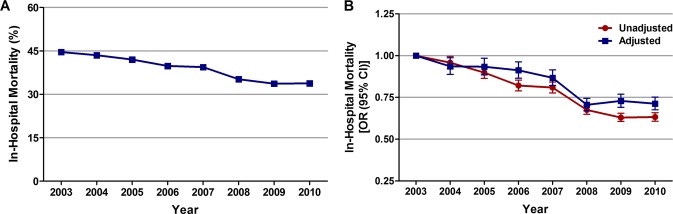
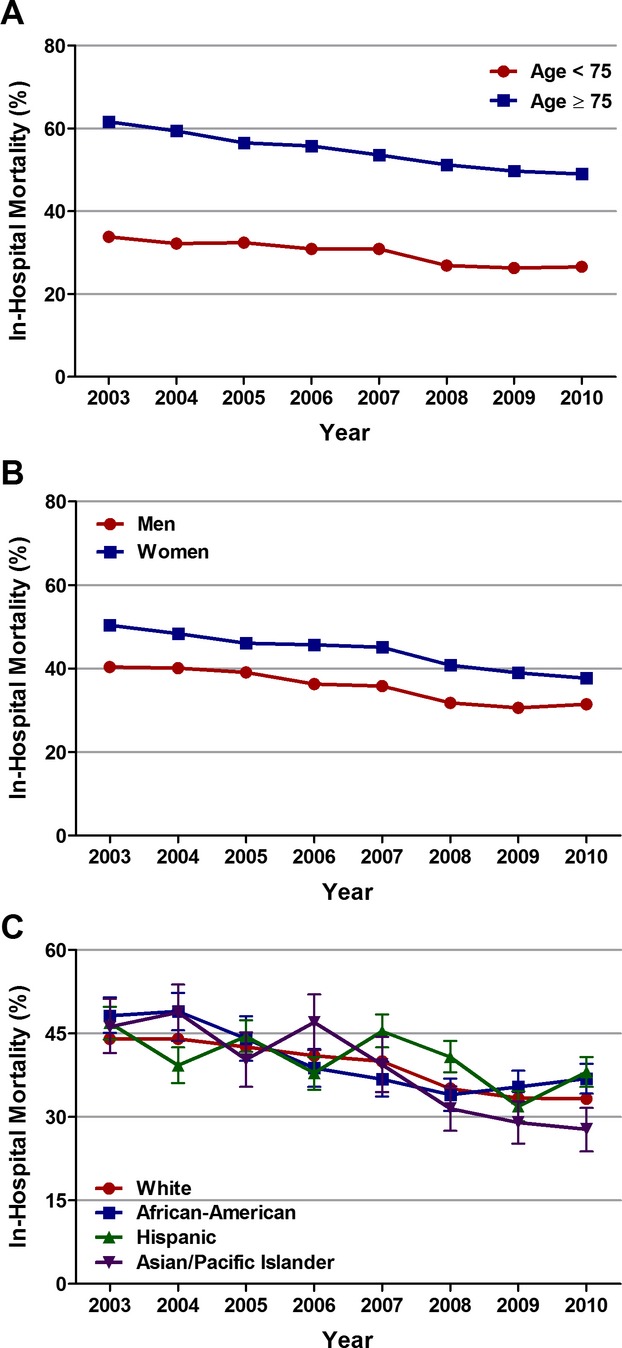
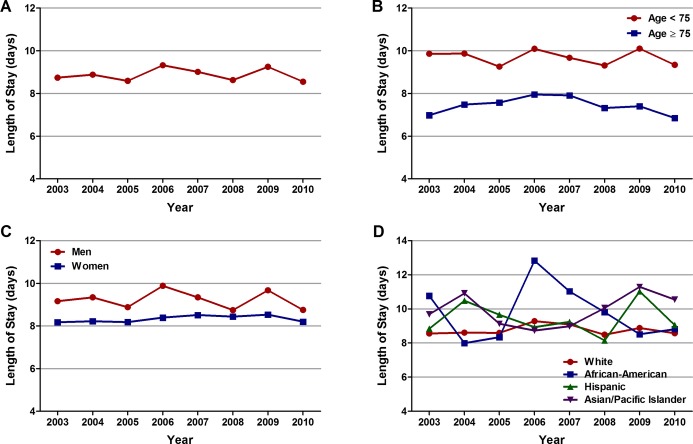
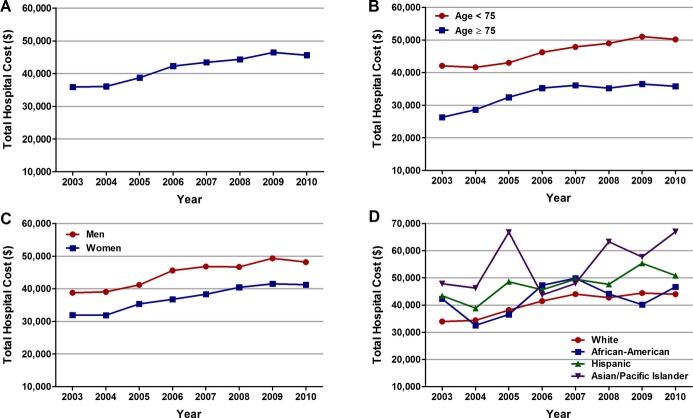
Methods and results: We queried the 2003-2010 Nationwide Inpatient Sample databases to identify all patients ≥ 40 years of age with STEMI and cardiogenic shock. Overall and age-, sex-, and race/ethnicity-specific trends in incidence of cardiogenic shock, early mechanical revascularization, and intra-aortic balloon pump use, and inhospital mortality were analyzed. From 2003 to 2010, among 1 990 486 patients aged ≥ 40 years with STEMI, 157 892 (7.9%) had cardiogenic shock. The overall incidence rate of cardiogenic shock in patients with STEMI increased from 6.5% in 2003 to 10.1% in 2010 (P(trend)<0.001). There was an increase in early mechanical revascularization (30.4% to 50.7%, P(trend)<0.001) and intra-aortic balloon pump use (44.8% to 53.7%, P(trend)<0.001) in these patients over the 8-year period. Inhospital mortality decreased significantly, from 44.6% to 33.8% (P(trend)<0.001; adjusted OR, 0.71; 95% CI, 0.68 to 0.75), whereas the average total hospital cost increased from $35 892 to $45 625 (P(trend)<0.001) during the study period. There was no change in the average length of stay (P(trend)=0.394). These temporal trends were similar in patients <75 and ≥ 75 years of age, men and women, and across each racial/ethnic group.
Conclusions: The incidence of cardiogenic shock complicating STEMI has increased during the past 8 years together with increased use of early mechanical revascularization and intra-aortic balloon pumps. There has been a concomitant decrease in risk-adjusted inhospital mortality, but an increase in total hospital costs during this period.
Keywords: ST‐elevation myocardial infarction; cardiogenic shock; early revascularization; inhospital mortality; trends.
Figures
References
-
- Goldberg RJ, Samad NA, Yarzebski J, Gurwitz J, Bigelow C, Gore JM. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999; 340:1162-1168 - PubMed
-
- Goldberg RJ, Gore JM, Thompson CA, Gurwitz JH. Recent magnitude of and temporal trends (1994–1997) in the incidence and hospital death rates of cardiogenic shock complicating acute myocardial infarction: the second national registry of myocardial infarction. Am Heart J. 2001; 141:65-72 - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999; 341:625-634 - PubMed
-
- Hochman JS, Sleeper LA, White HD, Dzavik V, Wong SC, Menon V, Webb JG, Steingart R, Picard MH, Menegus MA, Boland J, Sanborn T, Buller CE, Modur S, Forman R, Desvigne‐Nickens P, Jacobs AK, Slater JN, LeJemtel TH. One‐year survival following early revascularization for cardiogenic shock. JAMA. 2001; 285:190-192 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
