

Anti-epileptogenic clinical trial designs in epilepsy: issues and options
- PMID: 24420312
- PMCID: PMC3996121
- DOI: 10.1007/s13311-013-0252-z
Anti-epileptogenic clinical trial designs in epilepsy: issues and options
Abstract
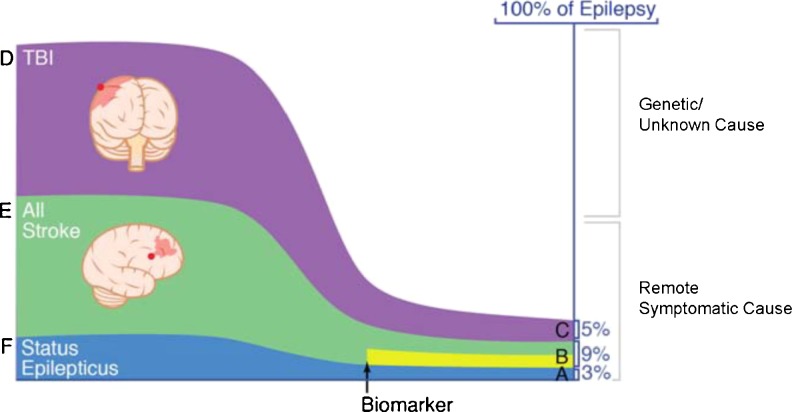
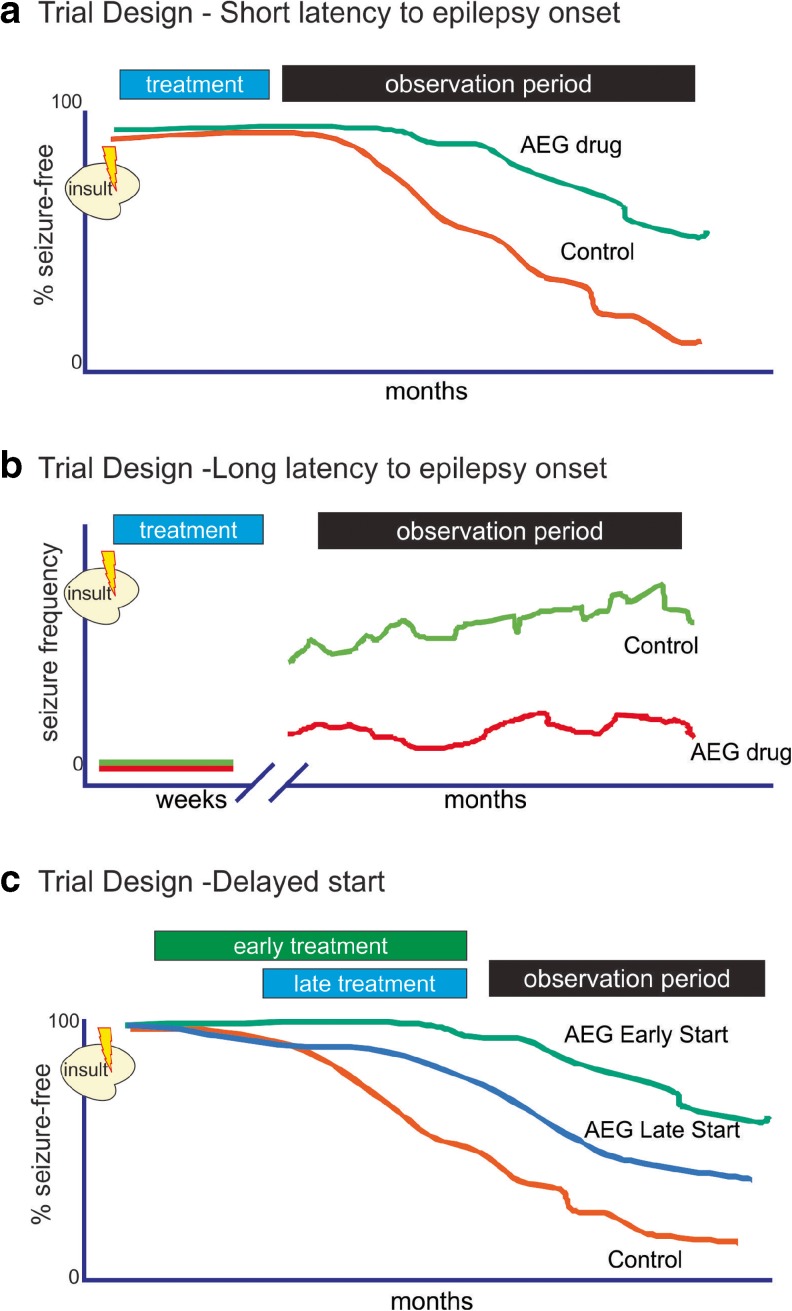
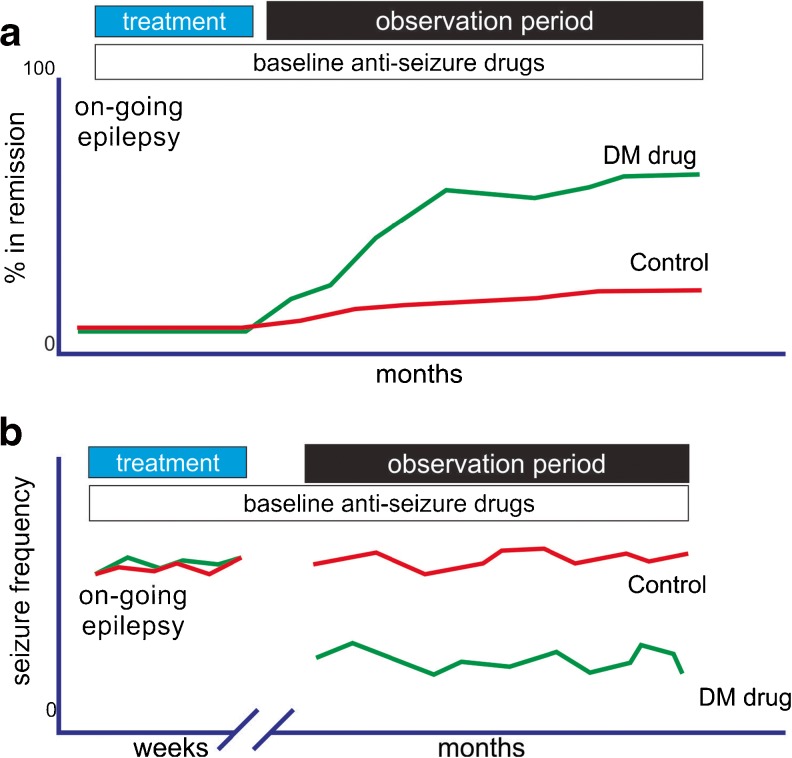
Although trials with anti-seizure drugs have not shown anti-epileptogenic or disease-modifying activity in humans, new compounds are on the horizon that may require novel trial designs. We briefly discuss the unique challenges and the available options to identify innovative clinical trial designs that differentiate novel anti-epileptogenic and disease-modifying compounds, preferably early in phase II, from current anti-seizure drugs. The most important challenges of clinical testing of agents for epilepsy prevention include having sufficient preclinical evidence for a suitable agent to proceed with a human trial of an anti-epileptogenic drug, and to demonstrate the feasibility of doing such a trial. Major challenges in trial design to assess agents for disease modification include the choice of suitable study parameters, the identification of a high-risk study population, the type of control, the time and duration of treatment, and a feasible follow-up period.
Figures
Similar articles
-
Clinical Trial Design for Disease-Modifying Therapies for Genetic Epilepsies.Neurotherapeutics. 2021 Jul;18(3):1445-1457. doi: 10.1007/s13311-021-01123-5. Epub 2021 Sep 30. Neurotherapeutics. 2021. PMID: 34595733 Free PMC article. Review.
-
New avenues for anti-epileptic drug discovery and development.Nat Rev Drug Discov. 2013 Oct;12(10):757-76. doi: 10.1038/nrd4126. Epub 2013 Sep 20. Nat Rev Drug Discov. 2013. PMID: 24052047 Review.
-
Inflammation and Epilepsy: Preclinical Findings and Potential Clinical Translation.Curr Pharm Des. 2017;23(37):5569-5576. doi: 10.2174/1381612823666170926113754. Curr Pharm Des. 2017. PMID: 28950818 Review.
-
Innovative clinical trial designs for future antiepileptic drugs.Epilepsia. 2007;48 Suppl 1:26-30. doi: 10.1111/j.1528-1167.2007.00996.x. Epilepsia. 2007. PMID: 17316410
-
Finding a better drug for epilepsy: preclinical screening strategies and experimental trial design.Epilepsia. 2012 Nov;53(11):1860-7. doi: 10.1111/j.1528-1167.2012.03541.x. Epub 2012 Jun 18. Epilepsia. 2012. PMID: 22708847 Free PMC article. Review.
Cited by
-
Thermosensitive, mucoadhesive brivaracetam nasal gel: a promising strategy for targeted relief of epilepsy.Naunyn Schmiedebergs Arch Pharmacol. 2025 Apr 26. doi: 10.1007/s00210-025-04172-1. Online ahead of print. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 40285836
-
Enhancing glymphatic fluid transport by pan-adrenergic inhibition suppresses epileptogenesis in male mice.Nat Commun. 2024 Nov 6;15(1):9600. doi: 10.1038/s41467-024-53430-y. Nat Commun. 2024. PMID: 39505840 Free PMC article.
-
Novel concepts in epileptogenesis and its prevention.Neurotherapeutics. 2014 Apr;11(2):229-30. doi: 10.1007/s13311-014-0268-z. Neurotherapeutics. 2014. PMID: 24652605 Free PMC article. No abstract available.
-
Increasing challenges to trial recruitment and conduct over time.Epilepsia. 2023 Oct;64(10):2625-2634. doi: 10.1111/epi.17716. Epub 2023 Jul 25. Epilepsia. 2023. PMID: 37440282 Free PMC article.
-
Brivaracetam in the treatment of epilepsy: a review of clinical trial data.Neuropsychiatr Dis Treat. 2019 Sep 9;15:2587-2600. doi: 10.2147/NDT.S143548. eCollection 2019. Neuropsychiatr Dis Treat. 2019. PMID: 31571877 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
