

Close antiplatelet therapy monitoring and adjustment based upon thrombelastography may reduce late-onset bleeding in HeartMate II recipients
- PMID: 24421208
- PMCID: PMC3957293
- DOI: 10.1093/icvts/ivt546
Close antiplatelet therapy monitoring and adjustment based upon thrombelastography may reduce late-onset bleeding in HeartMate II recipients
Abstract
Objectives: Bleeding is the most common complication of HeartMate II and is partially attributable to platelet dysfunction; however, antiplatelet therapy is arbitrary in most centres. We investigated how antiplatelet therapy adjustment with thrombelastography affects late-onset bleeding.
Methods: Thrombelastography was used to adjust antiplatelet therapy in 57 HeartMate II recipients. Kaplan-Meier survival curves and Cox proportional hazard ratio model were used to identify predictors of late-onset bleeding in univariate and multivariate analysis. Finally, late-onset bleeding rate in our study was compared with the reported rates in other studies in the literature, all of which did not use any test to monitor or adjust antiplatelet therapy.
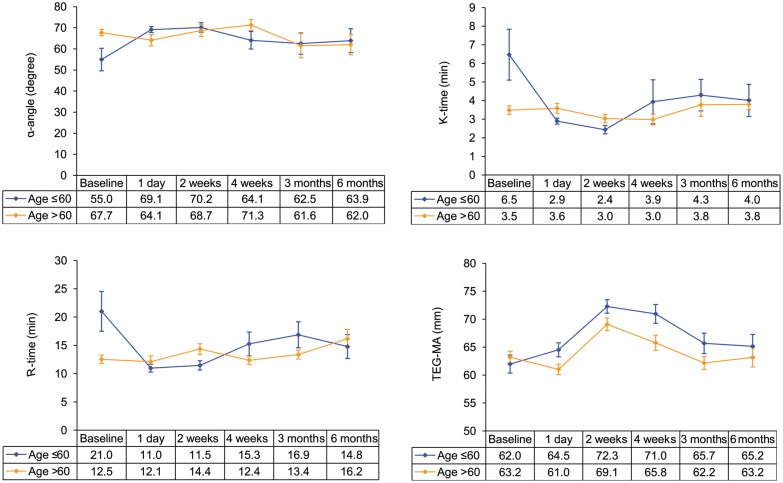
Results: Mean follow-up was 347 days. Eighteen late-onset bleeding events occurred in 12 patients, a late-onset bleeding rate of 12/57 (21%) or 0.21 events/patient-year. The Kaplan-Meier survival curves demonstrated that late-onset bleeding was more common in the destination therapy cohort (P = 0.02), in patients older than 60 years (P = 0.04) and in females (P = 0.01), none of which was significant in multivariate analysis at a significance level of 0.05. To further investigate the higher bleeding rate in elderly patients, thrombelastography parameters were compared between younger and older patients at the age cut-off of 60 years which demonstrated a prothrombotic change the day after device implantation in younger patients that was absent in the elderly. There was also a trend towards higher requirement for antiplatelet therapy in younger patients while on device support, but the difference did not reach statistical significance. The average late-onset or gastrointestinal bleeding rate among seven comparable studies in the literature that did not use any monitoring test to adjust antiplatelet therapy was 0.49 events/patient-year.
Conclusions: Our study implicates that antiplatelet therapy adjustment with thrombelastography may reduce late-onset bleeding rate in HeartMate II recipients. Bleeding was more common in the elderly recipients and analysis of thrombelastography data suggests that a less aggressive antiplatelet therapy regimen could potentially lower bleeding rate in this vulnerable population.
Keywords: Bleeding; HeartMate II; Stroke; Thrombelastography; Thromboembolism.
Figures



Comment in
-
eComment. Thrombus strikes back: promising role of thromboelastography for thromboembolic risk prediction in HeartMate II recipients.Interact Cardiovasc Thorac Surg. 2014 Apr;18(4):465. doi: 10.1093/icvts/ivu047. Interact Cardiovasc Thorac Surg. 2014. PMID: 24639183 Free PMC article. No abstract available.
Similar articles
-
eComment. Thrombus strikes back: promising role of thromboelastography for thromboembolic risk prediction in HeartMate II recipients.Interact Cardiovasc Thorac Surg. 2014 Apr;18(4):465. doi: 10.1093/icvts/ivu047. Interact Cardiovasc Thorac Surg. 2014. PMID: 24639183 Free PMC article. No abstract available.
-
Antiplatelet Therapy and Adverse Hematologic Events During Heart Mate II Support.Circ Heart Fail. 2016 Jan;9(1):e002296. doi: 10.1161/CIRCHEARTFAILURE.115.002296. Circ Heart Fail. 2016. PMID: 26721914
-
Pilot investigation of a novel testing strategy for bleeding in ventricular assist device recipients.J Heart Lung Transplant. 2012 Jul;31(7):750-6. doi: 10.1016/j.healun.2012.02.032. Epub 2012 Apr 25. J Heart Lung Transplant. 2012. PMID: 22538169 Clinical Trial.
-
What is the optimal anticoagulation in patients with a left ventricular assist device?Interact Cardiovasc Thorac Surg. 2012 Oct;15(4):733-40. doi: 10.1093/icvts/ivs297. Epub 2012 Jul 3. Interact Cardiovasc Thorac Surg. 2012. PMID: 22761118 Free PMC article. Review.
-
Thromboelastography-Guided Antiplatelet Therapy for Patients with Ischemic Cerebrocardiovascular Diseases: A Systematic Review and Meta-Analysis.Cerebrovasc Dis. 2025;54(3):398-408. doi: 10.1159/000539976. Epub 2024 Jul 4. Cerebrovasc Dis. 2025. PMID: 38964297
Cited by
-
eComment. Thrombus strikes back: promising role of thromboelastography for thromboembolic risk prediction in HeartMate II recipients.Interact Cardiovasc Thorac Surg. 2014 Apr;18(4):465. doi: 10.1093/icvts/ivu047. Interact Cardiovasc Thorac Surg. 2014. PMID: 24639183 Free PMC article. No abstract available.
-
Stroke and Intracranial Hemorrhage in HeartMate II and HeartWare Left Ventricular Assist Devices: A Systematic Review.Neurocrit Care. 2017 Aug;27(1):17-25. doi: 10.1007/s12028-017-0386-7. Neurocrit Care. 2017. PMID: 28324260
-
An introduction to point-of-care testing in extracorporeal circulation and LVADs.Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):516-521. doi: 10.1182/asheducation-2018.1.516. Hematology Am Soc Hematol Educ Program. 2018. PMID: 30504352 Free PMC article. Review.
-
Management of anticoagulation and antiplatelet therapy in patients with left ventricular assist devices.J Thromb Thrombolysis. 2015 Apr;39(3):337-44. doi: 10.1007/s11239-014-1162-6. J Thromb Thrombolysis. 2015. PMID: 25549823
-
The Incidence, Predictors and Outcomes of Gastrointestinal Bleeding in Patients with Left Ventricular Assist Device (LVAD).Dig Dis Sci. 2015 Dec;60(12):3697-706. doi: 10.1007/s10620-015-3743-4. Epub 2015 Jun 14. Dig Dis Sci. 2015. PMID: 26072320
References
-
- Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, et al. Advanced heart failure treated with continuousflow left ventricular assist device. N Engl J Med. 2009;361:2241–51. - PubMed
-
- Miller LW, Pagani FD, Russell SD, John R, Boyle AJ, Aaronson KD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med. 2007;357:885–96. - PubMed
-
- Pagani FD, Miller LW, Russell SD, Aaronson KD, John R, Boyle AJ, et al. Extended mechanical circulatory support with a continuous-flow rotary left ventricular assist device. J Am Coll Cardiol. 2009;54:312–21. - PubMed
-
- Boyle AJ, Russell SD, Teuteberg JJ, Slaughter MS, Moazami N, Pagani FD, et al. Low thromboembolism and pump thrombosis with the HeartMate II left ventricular assist device: analysis of outpatient anti-coagulation. J Heart Lung Transplant. 2009;28:881–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
