

A survey of the management of newborns with severe hemophilia in Canada
- PMID: 24421686
- PMCID: PMC3805619
- DOI: 10.1093/pch/18.4.189
A survey of the management of newborns with severe hemophilia in Canada
Abstract
Objective: To determine the practice patterns of Canadian hematologists and neonatologists/paediatricians who care for newborns with hemophilia, with regard to vitamin K administration, use of empirical clotting factor replacement therapy, neuroimaging and timing of hematology consultation.
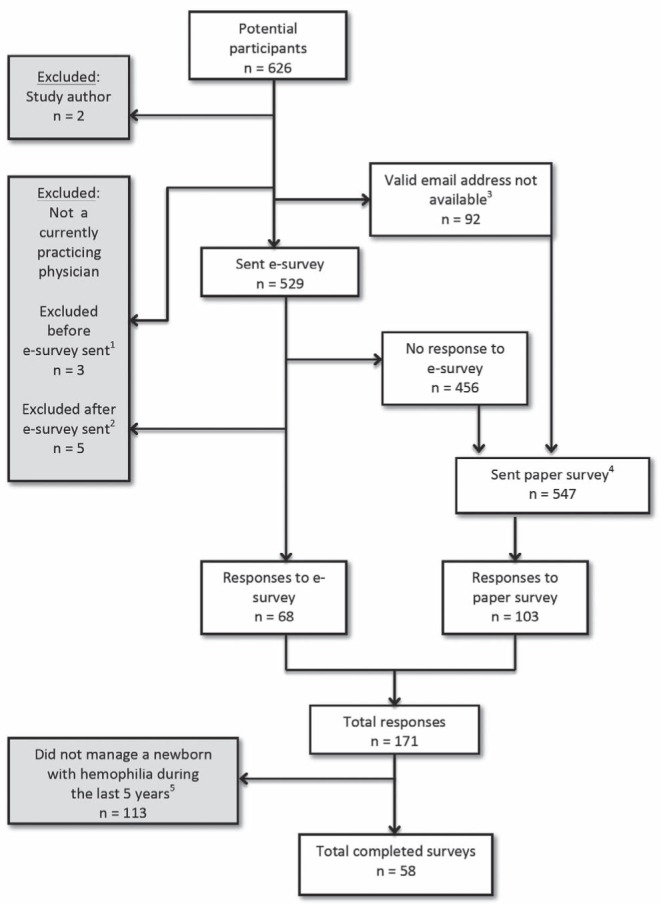
Methods: Hematologists and neonatologists/paediatricians, identified from membership lists of Canadian professional organizations, were provided electronic and/or paper versions of the survey instrument. Questions were posed in the context of specific clinical scenarios. Differences in response proportions between groups were compared for selected questions.
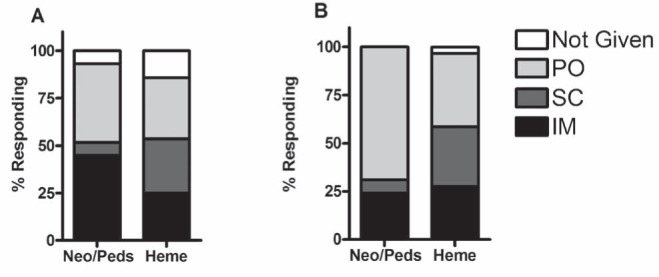
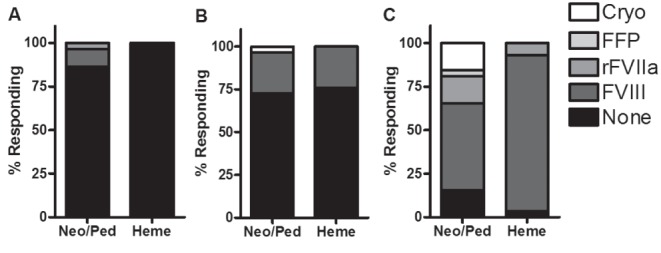
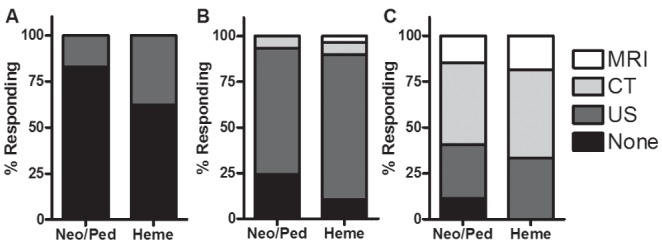
Results: There were 171 respondents among 616 eligible persons who were sent the survey; 58 respondents had recent experience managing a newborn with hemophilia. There was a consensus not to provide empirical treatment to well newborns after uncomplicated deliveries, to provide empirical treatment to symptomatic newborns and to obtain neuroimaging for symptomatic newborns. Systematic differences between hematologists and neonatologists/paediatricians existed with regard to the timing of hematology consultation when the diagnosis of hemophilia had not been confirmed antenatally, the route of vitamin K administration for newborns with hemophilia and the choice of product to use for empirical treatment of a symptomatic newborn.
Conclusions: The observed lack of consensus regarding important management decisions indicates a need for ongoing research in the care of newborns with hemophilia. Systematic differences between hematologists and neonatologists/paediatricians suggest a role for improved communication and collaboration between these two groups of practitioners.
Objectif: Déterminer les profils de pratique des hématologues et des néonatologistes/pédiatres canadiens qui soignent des nouveau-nés hémophiles à l’égard de l’administration de vitamine K, de l’utilisation empirique du traitement par le facteur de remplacement de coagulation, de la neuro-imagerie et du moment de la consultation en hématologie.
Méthodologie: Les hématologues et les néonatologistes/pédiatres, repérés grâce aux listes de membres d’organismes professionnels canadiens, ont reçu une version virtuelle, une version papier ou les deux versions du sondage. Les questions étaient posées dans le contexte de scénarios cliniques précis. Les différences dans les proportions de réponses entre les groupes étaient comparées à l’égard de questions sélectionnées.
Résultats: Sur les 616 personnes admissibles, 171 ont répondu au sondage. De ce nombre, 58 avaient eu une expérience récente de prise en charge d’un nouveau-né hémophile. On observait un consensus de ne pas administrer de traitement empirique aux nouveau-nés en santé après un accouchement sans complication, d’administrer un traitement empirique aux nouveau-nés symptomatiques et d’obtenir une neuroimagerie chez ces nouveau-nés symptomatiques. Il y avait des différences systématiques entre les hématologues et les néonatologistes/pédiatres pour ce qui est du moment de la consultation en hématologie lorsque le diagnostic n’avait pas été confirmé pendant la période anténatale, de la voie d’administration de la vitamine K aux nouveau-nés hémophiles et du choix de produit à utiliser pour administrer un traitement empirique à un nouveau-né symptomatique.
Conclusions: L’absence de consensus observé au sujet d’importantes décisions de prise en charge démontre la nécessité de poursuivre les recherches sur les soins aux nouveau-nés hémophiles. En raison des différences systématiques entre les hématologues et les néonatologistes/pédiatres, il y aurait lieu d’améliorer les communications et la collaboration entre ces deux groupes de praticiens.
Keywords: Hemophilia A; Hemophilia B; Intracranial hemorrhages; Neuroimaging; Newborn.
Figures
References
-
- Yoffe G, Buchanan GR. Intracranial hemorrhage in newborn and young infants with hemophilia. J Peds. 1988;113:333–6. - PubMed
-
- Stieltjes N, Calvez T, Demiguel V, et al. Intracranial haemorrhages in French haemophilia patients (1991–2001): Clinical presentation, management and prognosis factors for death. Haemophilia. 2005;11:452–8. - PubMed
-
- Miles BS, Anderson P, Agostino A, et al. Effect of intracranial bleeds on the neurocognitive, academic, behavioural and adaptive functioning of boys with haemophilia. Haemophilia. 2012;18:229–34. - PubMed
-
- James AH, Hoots K. The optimal mode of delivery for the haemophilia carrier expecting an affected infant is caesarean delivery. Haemophilia. 2010;16:420–4. - PubMed
-
- Ljung R. The optimal mode of delivery for the haemophilia carrier expecting an affected infant is vaginal delivery. Haemophilia. 2010;16:415–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources