

Are wait times and length of stay in Alberta emergency departments for children's mental health meeting national benchmarks? Trends from 2002 to 2008
- PMID: 24421704
- PMCID: PMC3680260
Are wait times and length of stay in Alberta emergency departments for children's mental health meeting national benchmarks? Trends from 2002 to 2008
Abstract
Objective: To describe wait times, treatment times and length of stay (LOS) for pediatric mental health visits to emergency departments (EDs).
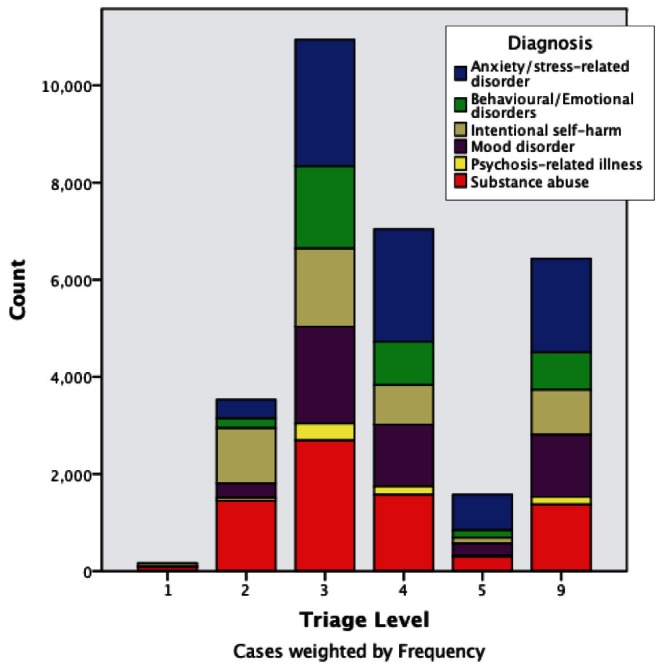
Methods: The present study was a retrospective cohort analysis of mental health visits (n=30,656) made by children <18 years of age between April 2002 and March 2008 to EDs in Alberta using administrative data. Wait time (time from triage to physician assessment), treatment time (time from physician assessment to end of visit) and LOS (time from start to end of visit) were examined for each visit. Wait time and treatment time data were available for 2006 to 2008, and LOS data were available for all study years. Wait times and LOS were compared with national benchmarks for the Canadian Triage and Acuity Scale (CTAS; levels 1 [resuscitative] through 5 [nonurgent]). All times are presented in h and min.
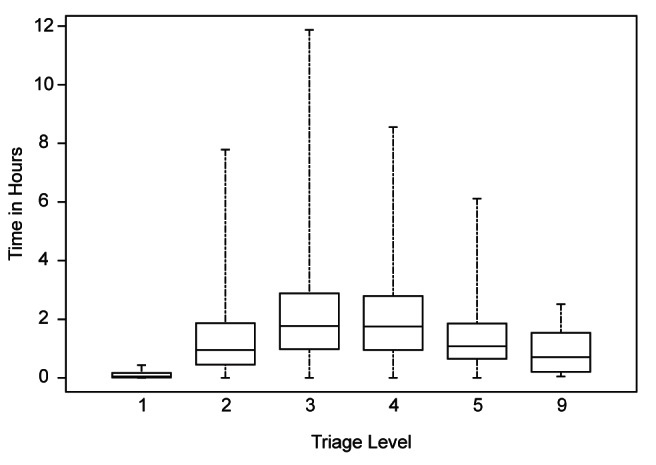
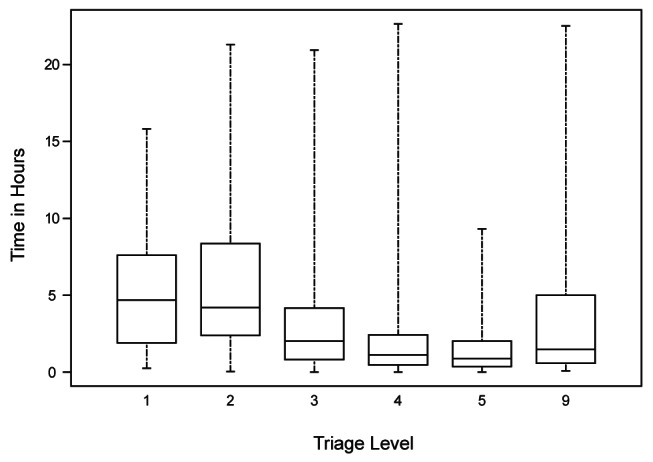
Results: Median wait times for visits triaged as CTAS 1, 2, 3 and 4 exceeded national recommendations. The longest wait times were for visits triaged as urgent (CTAS 3; 1 h 46 min) and less urgent (CTAS 4; 1 h 45 min). Lower-acuity visits had wait times that exceeded treatment times (CTAS 4: 1 h 45 min versus 1 h 8 min; CTAS 5: 1 h 5 min versus 52 min). Across all CTAS levels, the LOS in the ED increased during the study period, but met national benchmarks.
Conclusions: Most median ED wait times for pediatric mental health visits exceeded national recommendations, while the median LOS for all visits met recommendations. Lower-acuity visits had wait times that exceeded treatment times. Future research should explore whether longer wait times are associated with adverse outcomes, and whether current wait/treatment times are warranted to ensure that ED throughput is optimized.
Objectif: Décrire les temps d’attente, la durée du traitement et la durée de séjour (DdS) lors de visites au département d’urgence (DU) en raison de problèmes de santé mentale en pédiatrie.
Méthodologie: La présente étude était une analyse rétrospective de cohorte des visites effectuées par des enfants de moins de 18 ans pour des problèmes de santé mentale (n=30 656) entre avril 2002 et mars 2008 aux DU de l’Alberta, extrapolées selon les données administratives. Pour chaque visite, les chercheurs ont examiné le temps d’attente (délai entre le triage et l’évaluation du médecin), la durée du traitement (délai entre l’évaluation du médecin et la fin de la visite) et la DdS (délai entre le début et la fin de la visite). Les données sur le temps d’attente et la durée du traitement étaient disponibles de 2006 à 2008, tandis que celles sur la DdS l’étaient pour toutes les années de l’étude. Les chercheurs ont comparé les temps d’attente et la DdS avec les normes nationales d’après l’Échelle canadienne de triage et de gravité (ÉCTG; niveaux 1 [réanimation] à 5 [non urgent]). Les temps et les durées sont présentés en heures et en minutes.
Résultats: Le temps d’attente médian des visites dont le triage correspondait à une ÉCTG de 1, 2, 3 et 4 était supérieur aux recommandations nationales. Les temps d’attente les plus longs s’associaient aux visites classées comme urgentes (ÉCGT 3; 1 h 46 min) et moins urgentes (ÉCGT 4; 1 h 45 min) lors du triage. Le temps d’attente des visites moins aiguës était plus long que la durée de traitement (ÉCGT 4 : 1 h 45 min par rapport à 1 h 8 min; ÉCGT 5 : 1 h 5 min par rapport à 52 min). Dans tous les niveaux d’ÉCGT, la DdS au DU a augmenté pendant la période de l’étude, mais respectait les normes nationales.
Conclusion: La plupart des temps d’attente médians des visites au DU pour des problèmes de santé mentale en pédiatrie étaient plus longs que les recommandations nationales, tandis que la DdS médiane de toutes les visites respectait les recommandations. Les visites moins aiguës s’associaient à des temps d’attente plus longs que la durée de traitement. Les prochaines recherches devraient viser à déterminer si les temps d’attente plus longs s’associent à des effets indésirables et si le temps d’attente et la durée de traitement actuels se justifient pour assurer l’optimisation du cheminement au DU.
Keywords: Crisis intervention; Emergencies; Health services administration; Pediatrics.
Figures
Similar articles
-
Children's Mental Health Visits to the Emergency Department: Factors Affecting Wait Times and Length of Stay.Emerg Med Int. 2014;2014:897904. doi: 10.1155/2014/897904. Epub 2014 Jan 19. Emerg Med Int. 2014. PMID: 24563785 Free PMC article.
-
Homelessness and Emergency Department Use: Wait Time Disparities Across Triage Acuity Levels.Cureus. 2023 Nov 27;15(11):e49520. doi: 10.7759/cureus.49520. eCollection 2023 Nov. Cureus. 2023. PMID: 38161888 Free PMC article.
-
A determination of emergency department pre-triage times in patients not arriving by ambulance compared to widely used guideline recommendations.CJEM. 2017 Jul;19(4):265-270. doi: 10.1017/cem.2016.398. Epub 2016 Dec 5. CJEM. 2017. PMID: 27917744
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
-
A Comparison of Surgery Wait Times and Postoperative Length of Hospital Stay Among Patients with Brain Tumors by Country-Level Income and Healthcare System: A Systematic Review and Meta-analysis.World Neurosurg. 2023 Sep;177:152-164.e13. doi: 10.1016/j.wneu.2023.06.030. Epub 2023 Jun 16. World Neurosurg. 2023. PMID: 37331477 Review.
Cited by
-
Influence of demographic factors on prolonged length of stay in an emergency department.PLoS One. 2024 Mar 18;19(3):e0298598. doi: 10.1371/journal.pone.0298598. eCollection 2024. PLoS One. 2024. PMID: 38498485 Free PMC article.
-
Children's Mental Health Visits to the Emergency Department: Factors Affecting Wait Times and Length of Stay.Emerg Med Int. 2014;2014:897904. doi: 10.1155/2014/897904. Epub 2014 Jan 19. Emerg Med Int. 2014. PMID: 24563785 Free PMC article.
References
-
- Canadian Institute for Health Information (CIHI) Ottawa, Ontario: CIHI; 2005. Understanding emergency department wait times. Who is using emergency departments and how long are they waiting? < https://secure.cihi.ca/free_products/Wait_times_e.pdf> (Accessed April 17, 2012).
-
- Canadian Institute for Health Information (CIHI) Understanding emergency department wait times. How long to people spend in emergency departments in Ontario? Ottawa, Ontario: CIHI; Jan, 2007. < https://secure.cihi.ca/free_products/emergency_department_wait_times_e.pdf> (Accessed April 17, 2012).
-
- Canadian Association of Emergency Physicians (CAEP) Taking action on the issue of overcrowding in Canada’s emergency departments. CAEP. 2005 Jun 16; < www.waittimealliance.ca/waittimes/CAEP.pdf> (Accessed April 17, 2012).
-
- Liew D, Liew D, Kennedy MP. Emergency department length of stay independently predicts excess inpatient length of stay. Med J Aust. 2003;179:524–6. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous