

Traumatic portacaval shunt: a case report and literature review
- PMID: 24421924
- PMCID: PMC3888332
- DOI: 10.3941/jrcr.v7i11.1817
Traumatic portacaval shunt: a case report and literature review
Abstract
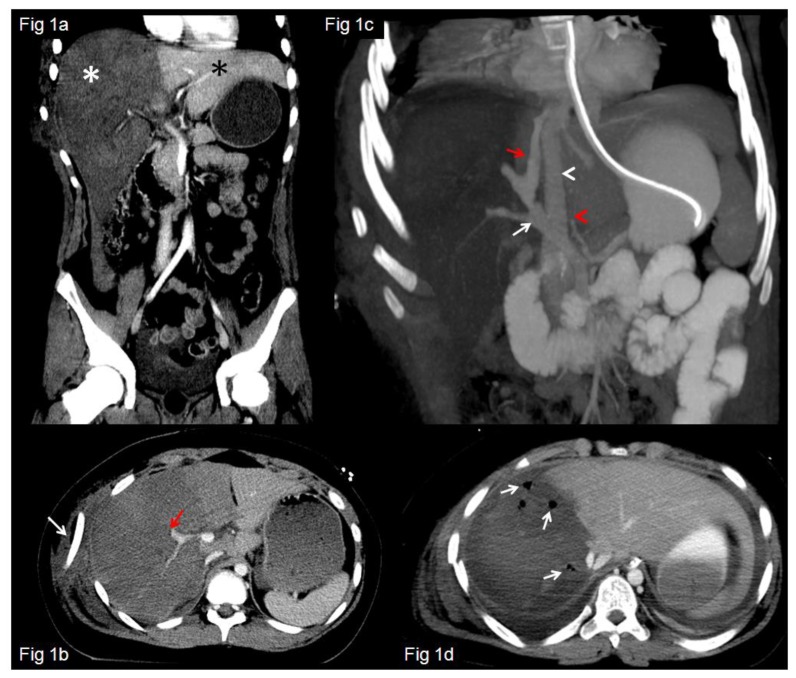
Computed tomography (CT) evaluation of the acute polytrauma patient has become well established as a mainstay of ER triage in hemodynamically stable patients. The radiologist plays a pivotal role in directing management by identifying and appropriately categorizing the severity of a patient's injuries. High-grade liver injuries have undergone an increasing trend of nonoperative management over the last several decades, with concurrent decrease in mortality. However, we present a case of a patient with a grade V liver laceration, in whom a rare portacaval shunt was also present. In the setting of this rare injury, the radiologist will likely be the first person to recognize and categorize a severe complication, which may indicate the need for a fundamental change in patient management.
Keywords: High grade liver injury; grade V liver laceration; traumatic portacaval fistula; traumatic portosystemic fistula; traumatic portosystemic shunt.
Figures



References
-
- Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. Organ Injury Scaling: Spleen and Liver (1994 Revision) J Trauma. 1995;38:323–4. - PubMed
-
- Kozar RA, Moore JB, Niles SE, Holcomb JB, Moore EE, Cothren CC, Hartwell E, Moore FA. Complications of Nonoperative Management of High-Grade Blunt Hepatic Injuries. J Trauma. 2005;59:1066–1071. - PubMed
-
- Ahn JH, Yu JS, Hwang SH, Chung JJ, Kim JH, Kim KW. Nontumorous arterioportal shunts in the liver: CT and MRI findings considering mechanisms and fate. Eur Radiol. 2010;20:385–394. - PubMed
-
- Guzman EA, McCahill LE, Rogers FB. Arterioportal fistulas: introduction of a novel classification with therapeutic implications. J Gastrointest Surg. 2006;10:543–550. - PubMed
-
- Bosoi CR, Rose CF. Brain edema in acute liver failure and chronic liver disease: Similarities and differences. Neurochem Int. 2013 Mar;62(4):446–57. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources