

Voriconazole-induced periostitis in two post-transplant patients
- PMID: 24421948
- PMCID: PMC3888175
- DOI: 10.3941/jrcr.v7i8.1458
Voriconazole-induced periostitis in two post-transplant patients
Abstract
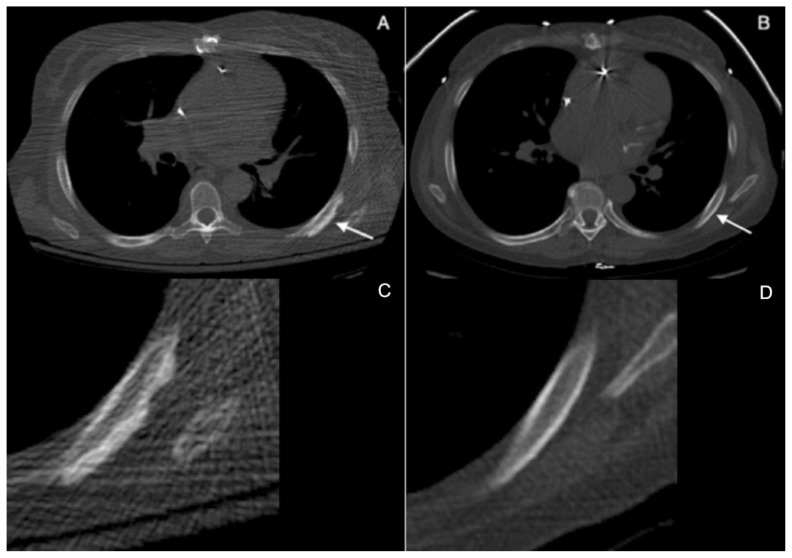
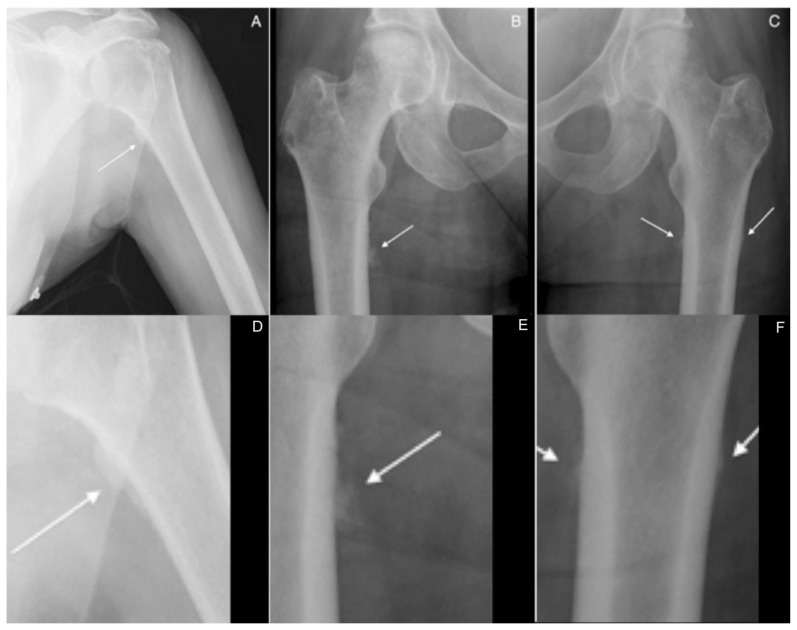
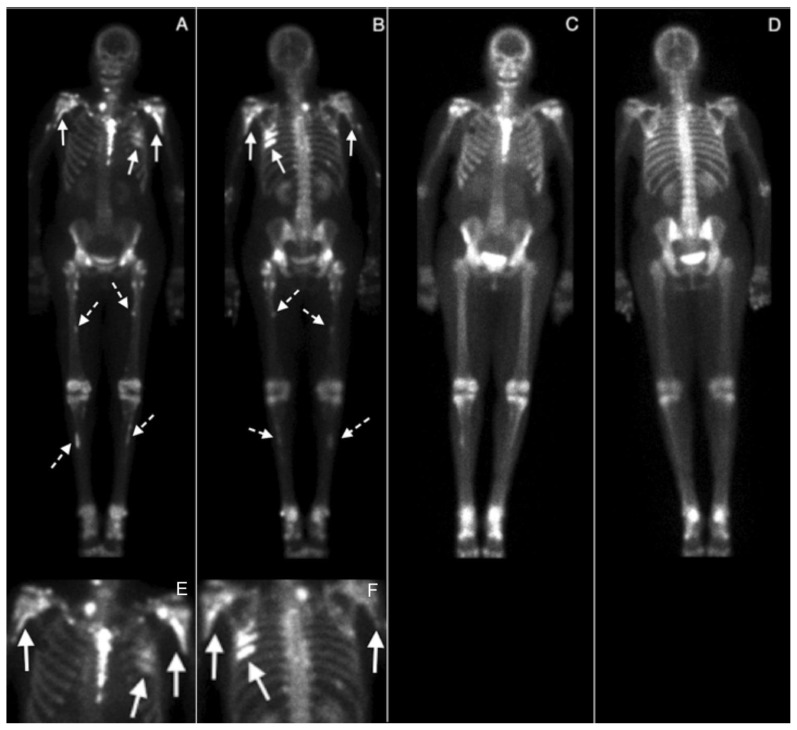
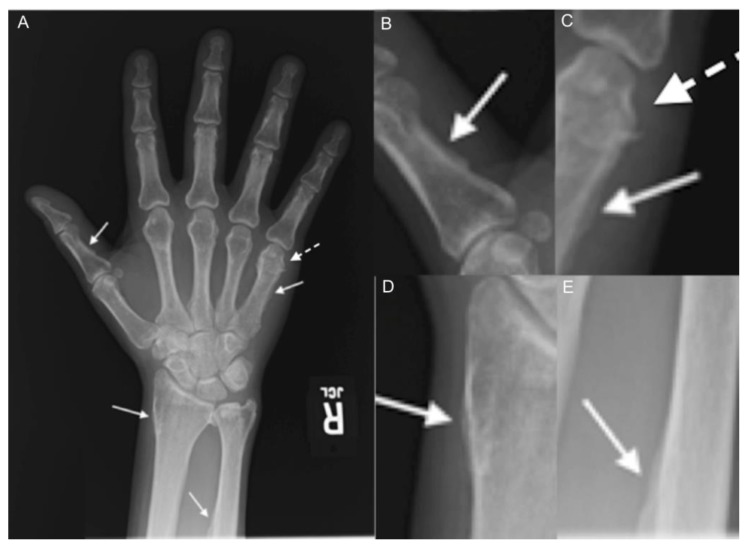
While drug-related periostitis has been known of for many years, the specific association of diffuse periostitis with voriconazole (most frequently in transplant patients) has only been recently explicitly addressed in the literature. Recognition of the radiologic and clinical manifestations of voriconazole-related periostitis is important for helping to narrow an otherwise broad differential diagnosis. We present two cases that illustrate different radiologic presentations of this painful cause of diffuse periostitis. Case 1 features a 60 year-old woman with a history of orthotopic heart transplant who was hospitalized for "full body pain" with progressively worsening bone tenderness involving the humeri, knees, femurs, hips, and hands. Case 2 describes a 48 year-old man with a history of acute lymphoblastic leukemia status post stem cell transplant who presented with diffuse arthralgias involving bilateral ankles, knees, wrists, and elbows.
Keywords: Periostitis deformans; hypertrophic osteoarthropathy; lung transplant; voriconazole.
Figures

References
-
- Gronblad M, et al. Innervation of human bone periosteum by peptidergic nerves. The Anatomical record. 1984 Jul;209(3):297–299. - PubMed
-
- Johnson LB, Kauffman CA. Voriconazole: a new triazole antifungal agent. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2003 Feb;36(5):630–637. - PubMed
-
- Ally R, et al. A randomized, double-blind, double-dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2001 Sep;33(9):1447–1454. - PubMed
-
- Singh N, Husain S. Aspergillus infections after lung transplantation: clinical differences in type of transplant and implications for management. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation. 2003 Mar;22(3):258–266. - PubMed
-
- Cahill BC, et al. Aspergillus airway colonization and invasive disease after lung transplantation. Chest. 1997 Nov;112(5):1160–1164. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources