

Case Reports
doi: 10.3941/jrcr.v7i9.1516.
eCollection 2013 Sep.
Posterior dislocation of long head of biceps tendon following traumatic anterior shoulder dislocation: imaging and intra-operative findings
Affiliations
- PMID: 24421954
- PMCID: PMC3888182
- DOI: 10.3941/jrcr.v7i9.1516
Item in Clipboard
Case Reports
Posterior dislocation of long head of biceps tendon following traumatic anterior shoulder dislocation: imaging and intra-operative findings
J Radiol Case Rep.
.
Abstract
A case of posterior dislocation of the long head of biceps tendon, a rare occurrence following traumatic anterior glenohumeral dislocation, along with complete rotator cuff rupture and large haemarthrosis is presented with imaging and intra-operative findings. The interposed tendon prevented complete reduction. Appearances at MRI were diagnostic and directed the surgical approach.
Keywords: MRI; Posterior dislocation long head biceps tendon; failed glenohumeral reduction; traumatic anterior glenohumeral dislocation.
Figures
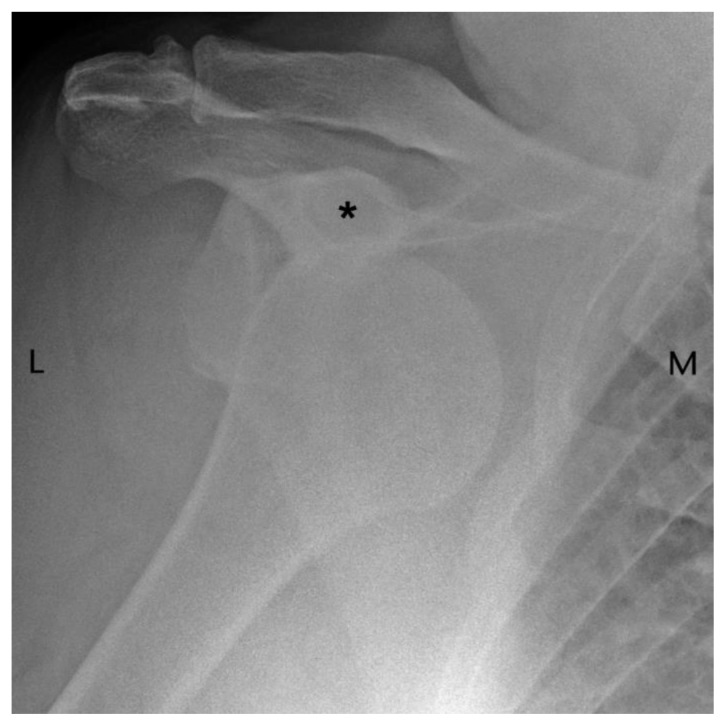
69 year old male presenting with traumatic anterior glenohumeral dislocation. Findings: the humeral head is seen to lie inferior to the coracoid process (asterisk) consistent with anterior shoulder dislocation. No definite fracture is seen. Technique: AP radiograph.
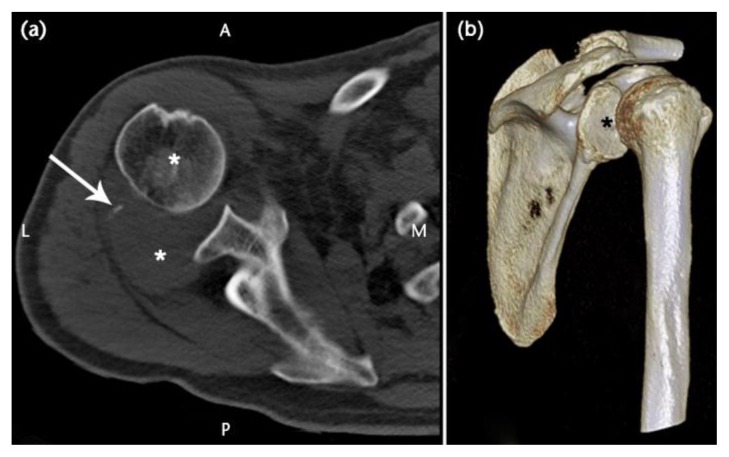
69 year old male with traumatic anterior glenohumeral dislocation. CT performed after failed attempts at reduction. Findings: a) axial image shows anterior subluxation at the glenohumeral joint, black asterisk marks humeral head. The course of infraspinatus is disrupted by a soft tissue “mass” posteriorly (posterior white asterisk) - a haemarthrosis within which lies a tiny avulsion fracture (arrow). b) Posterolateral view of a 3D volume reconstruction showing the relationship of the humerus to the glenoid fossa (asterisk). Technique: Unenhanced MDCT, 125 mAs, 120kV, slice thickness 1mm, increment 0.5 mm (Brilliance CT 64-channel, Philips, Surrey, UK).
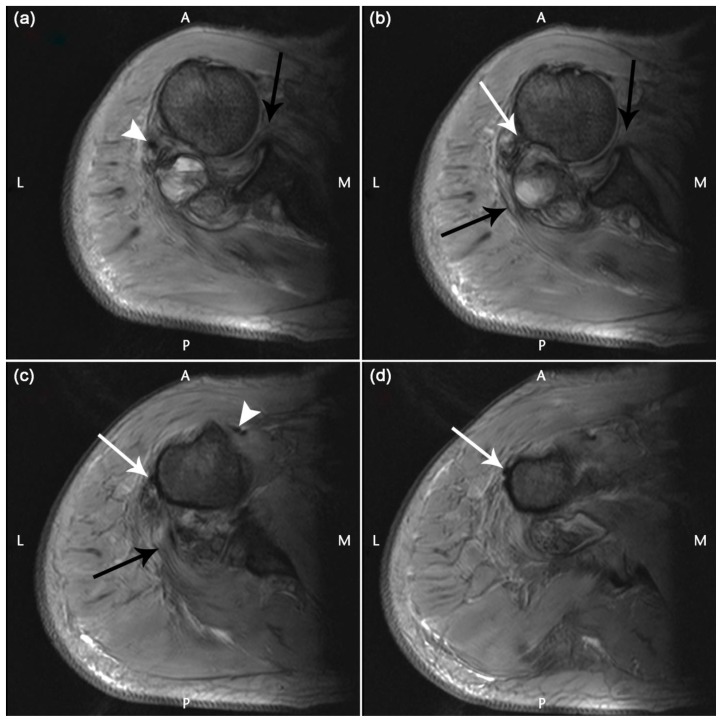
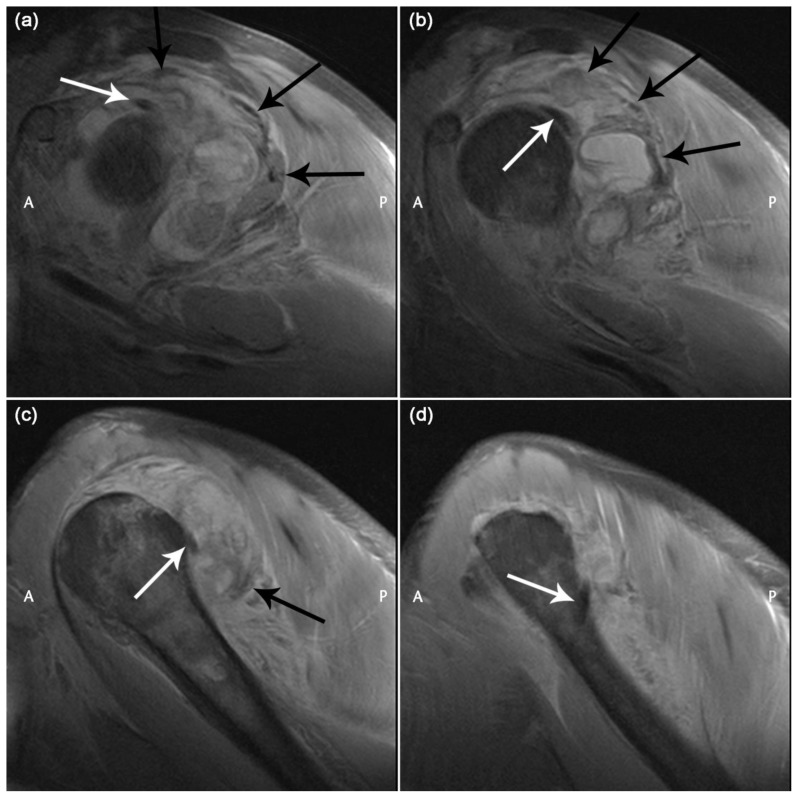
69 year old male with traumatic anterior glenohumeral dislocation with failed reduction after multiple attempts, complete rotator cuff tear, posterior dislocation long head of biceps tendon and haemarthrosis. Findings: a) There is an abnormal course of subscapularis with the disrupted tendon insertion folded into the anterior joint space (black arrow). A haemarthrosis with fluid-fluid levels is seen posterior to the joint. The tiny avulsion fracture, (white arrowhead) seen as a small hypointense focus lies posterolaterally. b) Disrupted subscapularis tendon and teres minor tendon are seen (anterior and posterior black arrows). The long head of biceps tendon has slipped over the greater tuberosity and lies posterior to the humeral head (white arrow). c) Disrupted teres minor insertion is demonstrated (black arrow). The dislocated long head of biceps tendon lies against the lateral aspect of humerus (white arrow). Short head of biceps can be seen (white arrowhead). d) The dislocated long head of biceps tendon is lying abnormally laterally at a more inferior level (white arrow). Technique: Axial gradient echo MRI a–d cranial to caudal 1.5T; TR/TE/Flip angle: 1300ms/27ms/30 degrees; FOV 200; matrix 410 × 512; slice thickness 4 mm.
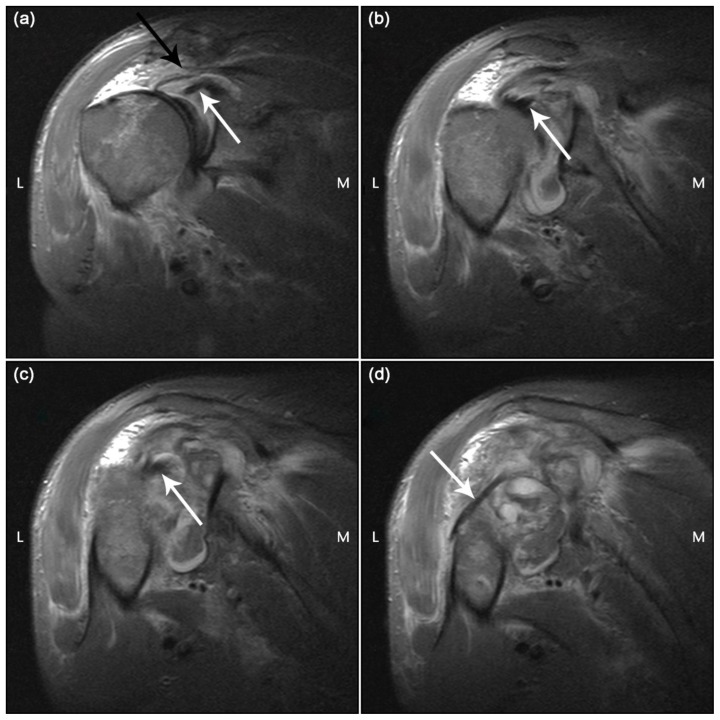
69 year old male with traumatic anterior glenohumeral dislocation with failed reduction after multiple attempts, complete rotator cuff tear, posterior dislocation long head of biceps tendon and haemarthrosis. Findings: a) The long head of biceps tendon can be seen at its origin on the superior glenoid (white arrow).There is a full-thickness tear of supraspinatus with retraction (black arrow). b) The intra-articular portion of the long head of biceps tendon is seen (white arrow). c) The long head of biceps tendon is lying posteriorly with respect to the bicipital groove (white arrow). d) The long head of biceps tendon can be seen dislocated posterior to the humerus (white arrow). Technique: Coronal oblique STIR anterior to posterior a–d 1.5T; TR/TE/time to inversion: 4290ms/29ms/130ms; FOV 160; matrix 394 × 512; slice thickness 4 mm
69 year old male with traumatic anterior glenohumeral dislocation with failed reduction after multiple attempts, complete rotator cuff tear, posterior dislocation long head of biceps tendon and haemarthrosis. Findings: a) The long head of biceps tendon is seen just lateral to its origin (white arrow). The musculotendinous portions of the rotator cuff: supraspinatus, infraspinatus and teres minor are seen in a clockwise direction (black arrows). b) The posteriorly dislocated long head of biceps tendon (white arrow) is seen. Torn, retracted supraspinatus demonstrated (superior black arrow) while infraspinatus and teres minor are stretched posteriorly due to the haemarthrosis (further black arrows). c) The posteriorly dislocated long head of biceps tendon is again seen (white arrow). Supraspinatus and infraspinatus are no longer seen. Torn teres minor is demonstrated (black arrow). d) The long head of biceps tendon is seen wrapping round the humeral shaft to come anteriorly (white arrow). No rotator cuff tendons are now visualised. Technique: Sagittal oblique proton-density medial to lateral a–d 1.5T; TR/TE: 3570ms/15ms; FOV 160; matrix 512 × 512; slice thickness 4 mm
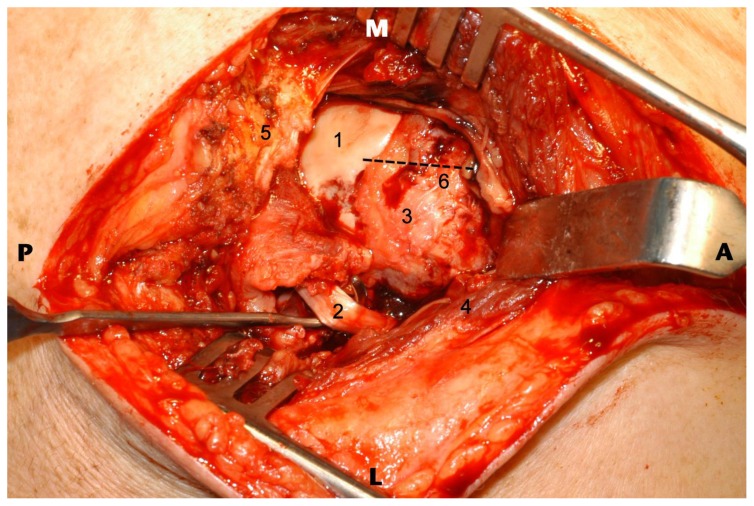
69 year old male following traumatic anterior glenohumeral dislocation with complete rotator cuff tear, posterior dislocation long head of biceps tendon and haemarthrosis at MRI. Intra-operative image seen as if from above, pre-reduction following removal of the haemarthrosis where tenotomy of long head of biceps tendon and rotator cuff repair were subsequently performed. Findings: 1) The exposed articular surface of the humeral head secondary to rotator cuff tear is seen. The humeral head remains anteriorly translated relative to the glenoid (and long head of biceps origin). 2) Posteriorly displaced long head of biceps tendon is shown by the Langenbeck retractor. 3) Supraspinatus footprint region. 4) Deltoid muscle (reflected during exposure) 5) Acromion is here. 6) Line of the bicipital groove and hence anatomical position of long head of biceps tendon. Technique: Superior strap approach with deltoid split.
Similar articles
-
Posterior dislocation of the long head biceps tendon: a case report, specific radiographic finding, and review of the literature.Skeletal Radiol. 2019 Jul;48(7):1131-1135. doi: 10.1007/s00256-018-3137-8. Epub 2019 Jan 5. Skeletal Radiol. 2019. PMID: 30612160 Review.
-
Anterior dislocation of the shoulder with rotator cuff injury and brachial plexus palsy: a case report.J Shoulder Elbow Surg. 2004 May-Jun;13(3):362-3. doi: 10.1016/j.jse.2003.12.011. J Shoulder Elbow Surg. 2004. PMID: 15111910 No abstract available.
-
Irreducible anterior dislocation of the shoulder due to soft tissue interposition of subscapularis tendon.Skeletal Radiol. 2008 Jan;37(1):63-5. doi: 10.1007/s00256-007-0370-y. Epub 2007 Oct 3. Skeletal Radiol. 2008. PMID: 17912520
-
Pseudoparalysis of shoulder caused by glenohumeral interposition of rotator cuff tendon stumps: a rare complication of posterior shoulder dislocation.Skeletal Radiol. 2013 Jan;42(1):135-9. doi: 10.1007/s00256-012-1478-2. Epub 2012 Jul 11. Skeletal Radiol. 2013. PMID: 22782290
-
Missed locked posterior shoulder dislocation with a reverse Hill-Sachs lesion and subscapularis rupture.Am J Orthop (Belle Mead NJ). 2013 Dec;42(12):E121-4. Am J Orthop (Belle Mead NJ). 2013. PMID: 24471154 Review.
Cited by
-
Posterior dislocation of the long head biceps tendon: a case report, specific radiographic finding, and review of the literature.Skeletal Radiol. 2019 Jul;48(7):1131-1135. doi: 10.1007/s00256-018-3137-8. Epub 2019 Jan 5. Skeletal Radiol. 2019. PMID: 30612160 Review.
-
Open reduction and rotator cuff repair of irreducible traumatic shoulder dislocation with sleeve-avulsion and glenohumeral interposition of the cuff: a case report and review of the literature.JSES Rev Rep Tech. 2022 May 23;2(3):399-405. doi: 10.1016/j.xrrt.2022.04.011. eCollection 2022 Aug. JSES Rev Rep Tech. 2022. PMID: 37588855 Free PMC article. No abstract available.
-
Long head of biceps in proximal fractures of the humerus: an underestimated problem?Acta Biomed. 2020 May 30;91(4-S):69-78. doi: 10.23750/abm.v91i4-S.9634. Acta Biomed. 2020. PMID: 32555078 Free PMC article. Review.
-
A massive rotator cuff tear in association with a posterior dislocation of the long head biceps tendon: a review of the literature on posterior long head biceps tendon dislocation.Skeletal Radiol. 2025 Jun 9. doi: 10.1007/s00256-025-04970-x. Online ahead of print. Skeletal Radiol. 2025. PMID: 40490587
-
Posterolateral dislocation and incarceration of the long head of the biceps tendon: a rare cause of irreducible anterior glenohumeral joint dislocation-a case report and brief review of the literature.Skeletal Radiol. 2024 Jun;53(6):1201-1204. doi: 10.1007/s00256-023-04468-4. Epub 2023 Oct 13. Skeletal Radiol. 2024. PMID: 37828097 Review.
References
-
- Nakata W, Katou S, Fujita A, Nakata M, Lefor AT, Sugimoto H. Biceps pulley: normal anatomy and associated lesions at MR arthrography. Radiographics. 2011;31:791–810. - PubMed
-
- Lee JC, Guy S, Connell D, Saifuddin A, Lambert S. MRI of the rotator interval of the shoulder. Clin Radiol. 2007;62:416–423. - PubMed
-
- Berbig R, Weishaupt D, Prim J, Shahin O. Primary anterior shoulder dislocation and rotator cuff tears. J Shoulder Elbow Surg. 1999;8:220–225. - PubMed
-
- Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am. 2012;94:18–26. - PubMed
-
- Bauer T, Vuillemin A, Hardy P, Rousselin B. Posterior dislocation of the long head of the biceps tendon: a case report. J Shoulder Elbow Surg. 2005;14:557–558. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical