

Effects of proteasome inhibitors on bone cancer
- PMID: 24422114
- PMCID: PMC3817984
- DOI: 10.1038/bonekey.2013.129
Effects of proteasome inhibitors on bone cancer
Abstract
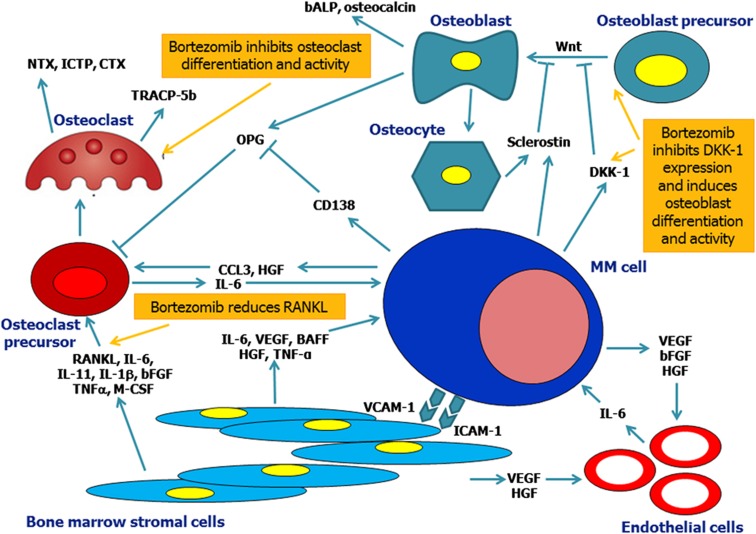
Bone metastasis is a frequent complication of cancer, occurring in up to 70% of patients with advanced breast or prostate cancer, while bone disease is also the characteristic clinical feature of multiple myeloma. Skeletal-related events can be devastating, with major effect on the quality of life and survival. Bisphosphonates are the mainstay of therapeutic management of bone disease of solid tumors and myeloma, and denosumab has recently been approved for patients with bone metastases. Both act through inhibition of the osteoclast activity but do not restore bone formation. Proteasome inhibition has direct bone anabolic effects. Proteasome inhibitors have been used in the management of patients with multiple myeloma and mantle-cell lymphoma during the last decade. In multiple myeloma, bortezomib, the first-in-class proteasome inhibitor, has shown both in vitro and in vivo regulation of bone remodeling by inhibiting osteoclast function and promoting osteoblast activity. Bortezomib also reduces bone resorption but more importantly increases bone formation and bone mineral density, at least, in subsets of myeloma patients. Thus, bortezomib is recommended for myeloma patients with extended bone disease in combination with bisphosphonates. This review focuses on the effects of the proteasome system on bone metabolism and the implications into the better management of patients with cancer and bone disease.
Conflict of interest statement
Evangelos Terpos declares honoraria and advisory fees from Janssen-Cilag. Dimitrios Christoulas has no interests to declare for this paper.
Figures
References
-
- Mackiewicz-Wysocka M, Pankowska M, Wysocki PJ. Progress in the treatment of bone metastases in cancer patients. Expert Opin Investig Drugs 2012; 21:785–795. - PubMed
-
- Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc 2003; 78:21–33. - PubMed
-
- Christoulas D, Terpos E, Dimopoulos MA. Pathogenesis and management of myeloma bone disease. Expert Rev Hematol 2009; 2:385–398. - PubMed
-
- Abe M, Hiura K, Wilde J, Shioyasono A, Moriyama K, Hashimoto T et al. Osteoclasts enhance myeloma cell growth and survival via cell-cell contact: a vicious cycle between bone destruction and myeloma expansion. Blood 2004; 104:2484–2491. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources