

A rare case of primary cardiac B cell lymphoma
- PMID: 24422789
- PMCID: PMC4021862
- DOI: 10.1186/1749-8090-9-14
A rare case of primary cardiac B cell lymphoma
Abstract
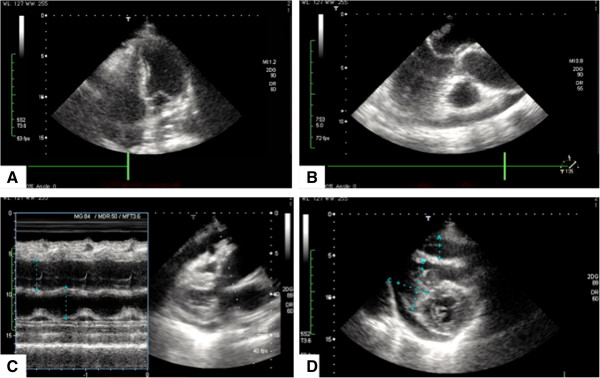
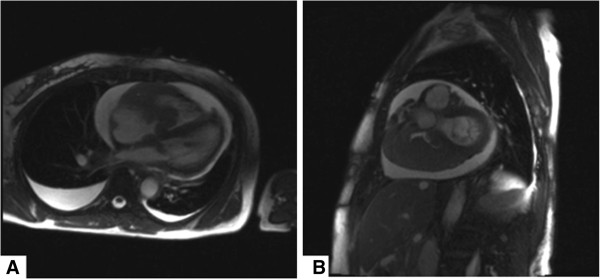
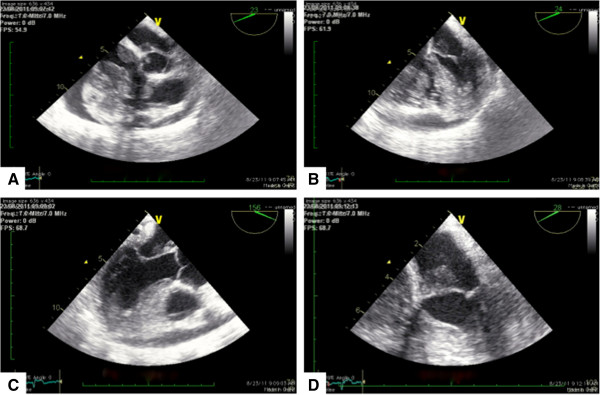
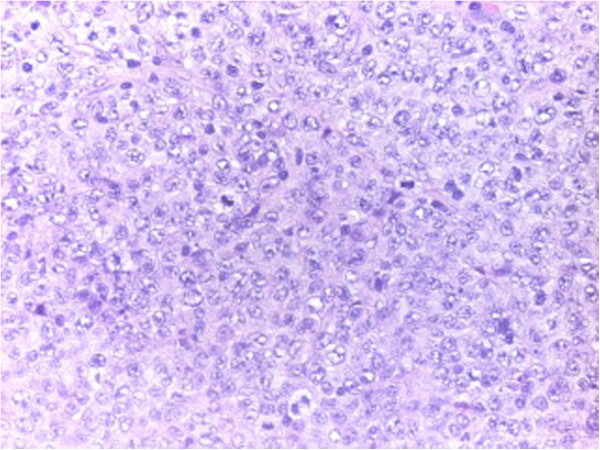
Primary cardiac lymphomas represent an extremely rare entity of extranodal lymphomas and should be distinguished from secondary cardiac involvement of disseminated lymphomas belonging to the non-Hodgkin's classification of blood cancers. Only 90 cases have been reported in literature. Presentation of cardiac lymphomas on imaging studies may not be unambiguous since they potentially mimic other cardiac neoplasms including myxomas, angiosarcoma or rhadomyomas and therefore require multimodality cardiac imaging, endomyocardial biopsy, excisional intraoperative biopsy and pericardial fluid cytological evaluation to establish final diagnosis.Herein we report the case of a 70 y/o immunocompetent Caucasian female with a rapidly progressing superior vena cava syndrome secondary to a large primary cardiac diffuse large B cell lymphoma (NHL lymphoma) almost completely obstructing the right atrium, right ventricle and affecting both mitral and tricuspid valve. The patient had no clinical evidence of disseminated disease and was successfully treated with extensive debulking during open-heart surgery on cardiopulmonary bypass and 6 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone chemotherapy (R-CHOP).
Figures
References
-
- McAllister HA Jr, Hall RJ, Cooley DA. Tumors of the heart and pericardium. Curr Prob Cardiol. 1999;9(2):57–116. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
