

Review
doi: 10.1146/annurev-immunol-032713-120136.
Epub 2014 Jan 9.
Adoptive immunotherapy for cancer or viruses
Affiliations
- PMID: 24423116
- PMCID: PMC4533835
- DOI: 10.1146/annurev-immunol-032713-120136
Item in Clipboard
Review
Adoptive immunotherapy for cancer or viruses
Annu Rev Immunol.
2014.
Abstract
Adoptive immunotherapy, or the infusion of lymphocytes, is a promising approach for the treatment of cancer and certain chronic viral infections. The application of the principles of synthetic biology to enhance T cell function has resulted in substantial increases in clinical efficacy. The primary challenge to the field is to identify tumor-specific targets to avoid off-tumor, on-target toxicity. Given recent advances in efficacy in numerous pilot trials, the next steps in clinical development will require multicenter trials to establish adoptive immunotherapy as a mainstream technology.
Figures
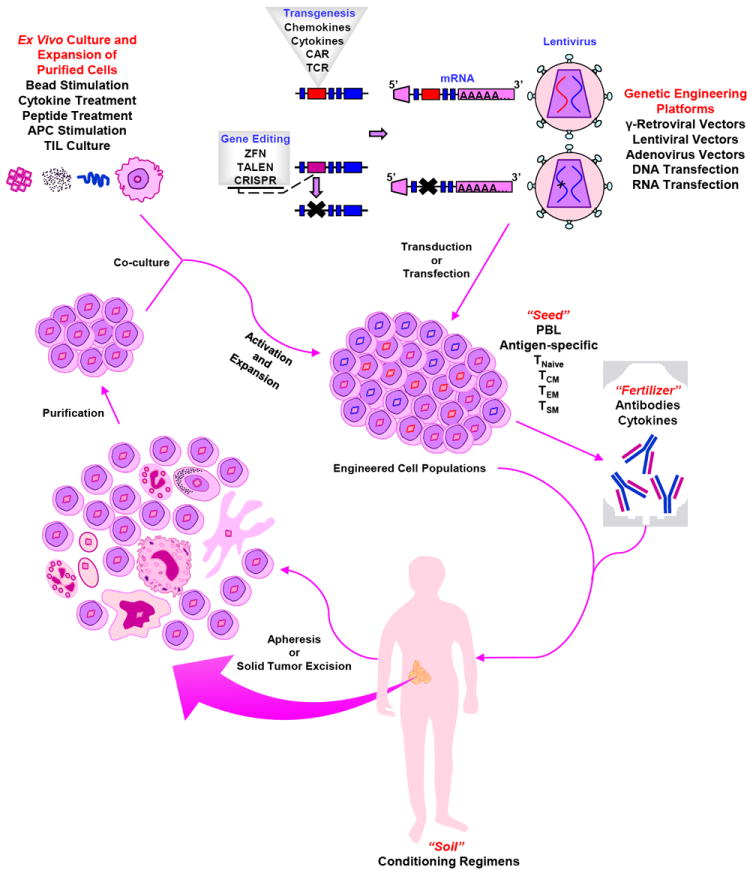
Autologous cells are harvested from the patient by apheresis. Following purification, cells undergo polyclonal in vitro activation and expansion, as well as genetic modification to form the “seed.” Engineered cell populations (“seeds”) are re-infused (“planted”) into the pre-conditioned patient (“soil”), along with antibodies and/or cytokines (“fertilizer”).
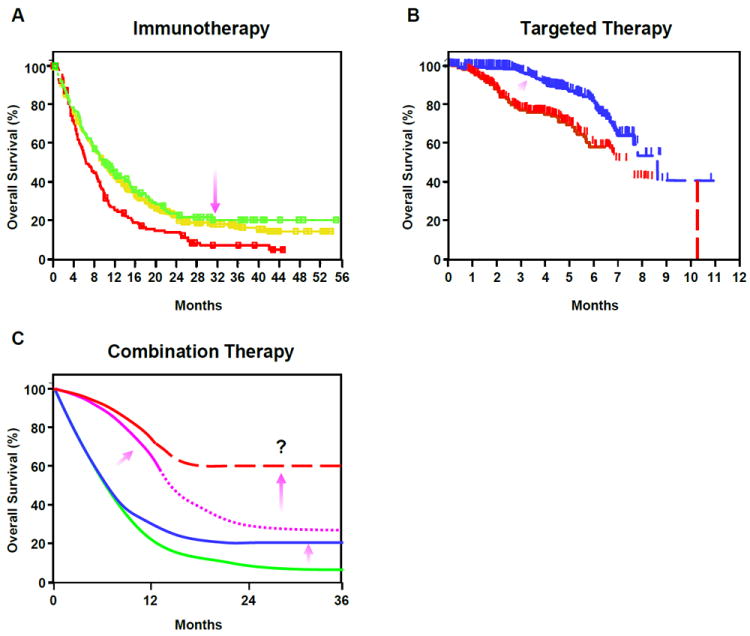
(A) Patients with metastatic melanoma exhibit improved survival with Ipilimumab treatment(23) (Kaplan-Meir survival plot). Treatments are as follows: ipilimumab-alone (green line); gp100-alone (red line); ipilimumab + gp100 (yellow line). Purple arrow indicates how immunotherapy raises the tail of curve, indicating prolonged effects. (B) Kaplan-Meir survival plot showing that improved survival can be achieved in melanoma with Vemurafenib therapy (204). Patients were treated with either Dacarbazine (red line) or Vemurafenib (blue line). Purple arrow indicates direction of change effected by targeted therapy; overall survival is improved early but effects are transient. (C) Hypothetically, the combination of immunotherapy with targeted treatment may increase survival in patients with metastatic cancers. The green line depicts a typical survival curve for standard cancer therapy; the blue line represents survival with immunotherapy alone; the purple line represents the effect of a targeted therapy alone survival plot; the dashed red line depicts the potential enhanced survival that can be achieved using immunotherapy combined with targeted therapy. Arrows highlight the impact of the above therapeutic regimens on the tail of the curve or the spread between curves for different treatments. Thus, immunotherapy requires more time, but increases survival; Targeted therapy works rapidly, but is not durable. Combining these strategies may ultimately improve the fraction of patients with long-term survival.
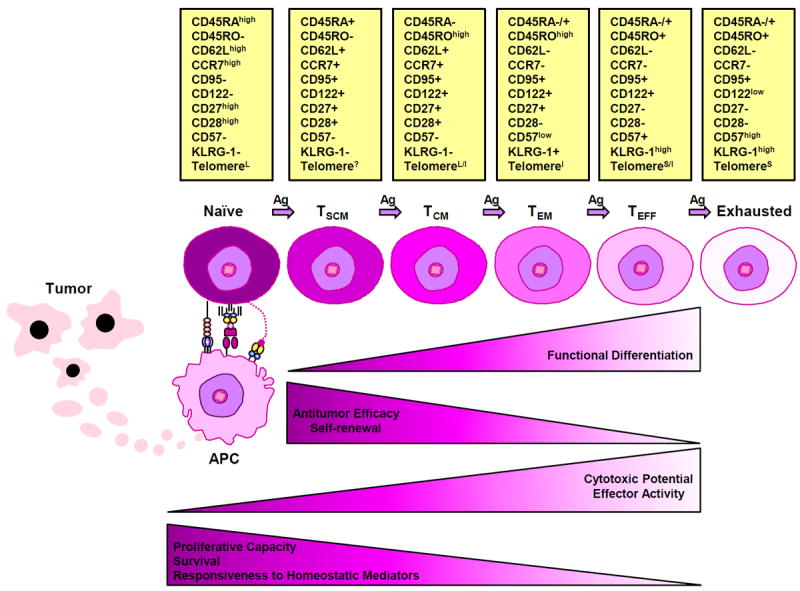
A state of persistent and frequent antigenic stimulation, such as that induced by tumor burden, facilitates a progressive differentiation pathway whereby naïve T cells become terminally differentiated effectors. Changes in the phenotypic markers that characterize progressive T cell differentiation are depicted as: expressed (+), not expressed (-), expressed at high levels (high), expressed at low levels (low); long telomere length (L), unknown telomere length (?); long/intermediate telomere length (L/I), intermediate telomere length (I), short/intermediate telomere length (S/I) and short telomere length (S). Together with the gradual shortening of telomere length, T cells lose their proliferative and self-renewal capacities, as well as responsiveness to homeostatic mediators and ultimately become exhausted. Although cytotoxic potential/effector functions increase with persistent antigen stimulation and T cells must be fully differentiated to possess anti-tumor activity, experimental evidence suggests that in the context of adoptive cell therapy, increasing differentiation state is inversely correlated with anti-tumor efficacy (205).
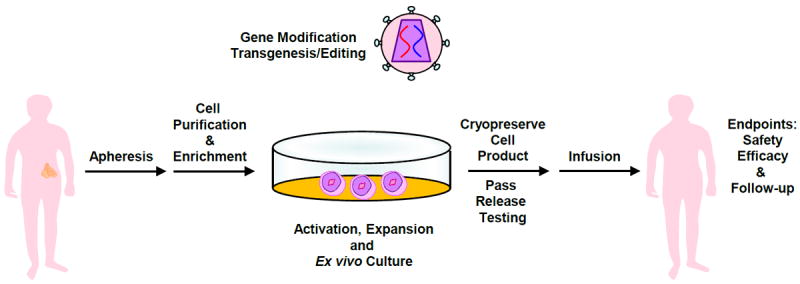
Cells of interest are isolated from the whole blood of a patient, followed by enrichment, activation and expansion. At the time of activation, the lentiviral vector is added. On the final day of culture, cells are harvested and cryopreserved in an infusible media. The patient is infused with gene-modified cells and endpoint assays are conducted at designated time intervals. At the conclusion of active monitoring, in the US, the patient is transferred to a destination protocol for long-term follow-up as per FDA guidelines.
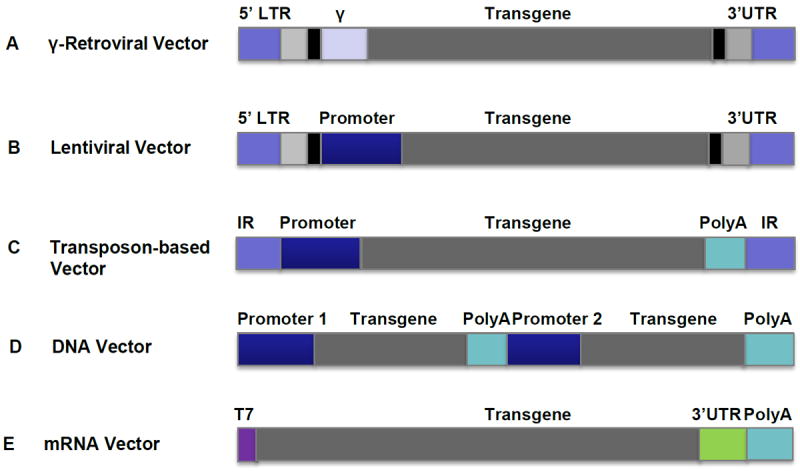
(A) γ-retroviral vectors are one of the most commonly used vector systems for permanent gene expression in T cells for adoptive immunotherapy in the clinic. Clinical grade vector produced under Good Manufacturing Practices (GMP) viral vectors can be produced by stable packaging cell lines. vectors. GMP Viral vectors can be produced by stable packaging lines. (B) Lentiviral vectors are becoming more popular vector systems for permanent gene expression in T cells for adoptive immunotherapy clinical trials, due to their advantages of transducing non-dividing cells, high transduction efficiency and potentially safer integrating profile over γ-Retroviral vectors. (C) Non-viral transposase-mediated gene transfer, in which gene integration is achieved by the provision of the transposase enzyme, can mediate permanent gene expression in T cells. (D) DNA can be directly transfected into T cells by electroporation and integrated; genetically modified T cells can be cloned and expanded. (E) T cells can be directly transfected by electroporation with in vitro transcribed mRNA without integrating. This is a transient transgene system and the transgene can be expressed in T cells for up to 1 week. Repeated infusions of the mRNA-transfected T cells are required. All vectors are depicted as linear DNA. Internal repeat (IR); Long terminal repeat (LTR); Packaging Signal (ψ); Untranslated region (UTR); Poly(A) tail (PolyA).
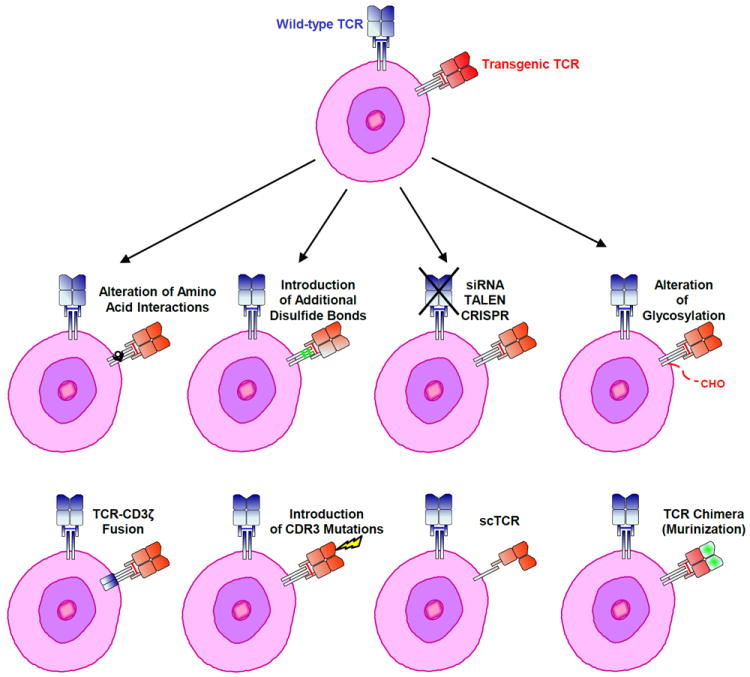
Expression of a transgenic TCR may be improved by preventing the formation of mixed dimers between endogenous and ectopic engineered TCR chains. These strategies include the alteration of amino acid interactions, the creation of TCR-CD3 ζ fusions, single chain (sc) receptors, TCR chimeras (murinization) and the introduction of additional disulfide bonds or glycosylation. Mutating amino acids in the complementarity determining region 3 (CDR3) and knocking down/out endogenous TCR expression may also increase transgenic TCR activity.
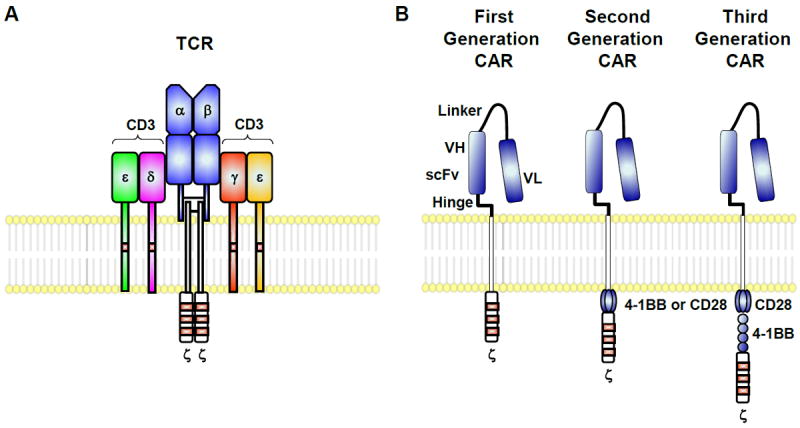
(A) Endogenous T cells express a single TCR. (B) Alternatively, these genes can be engineered to express chimeric tumor antigen–specific receptors or “CARs” that target surface antigens in an MHC-independent manner. T bodies express an extracellular portion that is usually derived from an antibody and intracellular signaling modules derived from T cell signaling proteins. First generation CARs contain CD3ζ, while second generation CARs possess a co-stimulatory endodomain (e.g., CD28 or 4-1BB) fused to CD3ζ. Third generation CARs consist of two co-stimulation endodomains linked to CD3ζ.
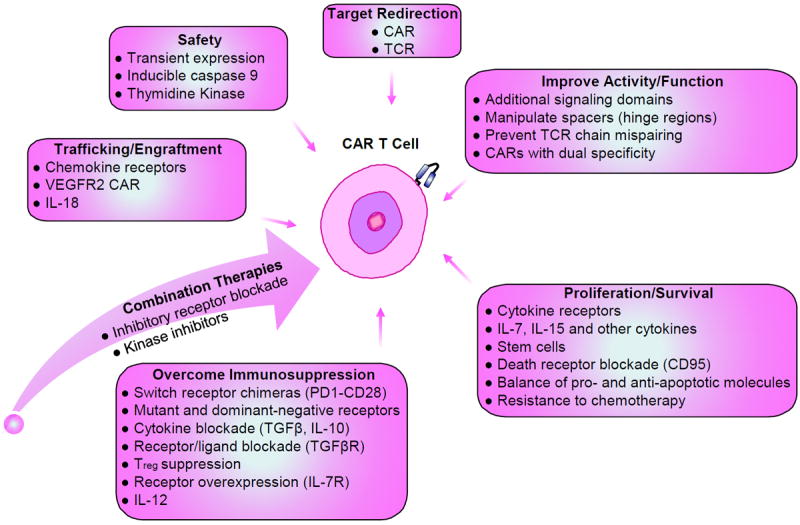
Various strategies can be undertaken to genetically modify T cells for adoptive therapy in an endeavor to enhance function and survival, proliferation, trafficking to tumor sites, and safety. Through genetic modification, these cells may also be armed to be efficacious in the immunosuppressive tumor microenvironment. Combination therapy can be used to improve the therapeutic efficacy of engineered T cells.
References
-
- Anderson WF. Prospects for human gene therapy. Science. 1984;226:401–9. - PubMed
-
- Friedmann T. A brief history of gene therapy. Nat Genet. 1992;2:93–8. - PubMed
-
- Mitsuyasu RT, Anton PA, Deeks SG, Scadden DT, Connick E, Downs MT, Bakker A, Roberts MR, June CH, Jalali S, Lin AA, Pennathur-Das R, Hege KM. Prolonged survival and tissue trafficking following adoptive transfer of CD4zeta gene-modified autologous CD4(+) and CD8(+) T cells in human immunodeficiency virus-infected subjects. Blood. 2000;96:785–93. - PubMed
-
- Deeks SG, Wagner B, Anton PA, Mitsuyasu RT, Scadden DT, Huang C, Macken C, Richman DD, Christopherson C, June CH, Lazar R, Broad DF, Jalali S, Hege KM. A phase II randomized study of HIV-specific T-cell gene therapy in subjects with undetectable plasma viremia on combination antiretroviral therapy. Mol Ther. 2002;5:788–97. - PubMed
-
- Scholler J, Brady TL, Binder-Scholl G, Hwang WT, Plesa G, Hege KM, Vogel AN, Kalos M, Riley JL, Deeks SG, Mitsuyasu RT, Bernstein WB, Aronson NE, Levine BL, Bushman FD, June CH. Decade-long safety and function of retroviral-modified chimeric antigen receptor T cells. Sci Transl Med. 2012;4:132ra53. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
