

Effects of testosterone and growth hormone on the structural and mechanical properties of bone by micro-MRI in the distal tibia of men with hypopituitarism
- PMID: 24423356
- PMCID: PMC3973782
- DOI: 10.1210/jc.2013-3665
Effects of testosterone and growth hormone on the structural and mechanical properties of bone by micro-MRI in the distal tibia of men with hypopituitarism
Abstract
Context: Severe deficiencies of testosterone (T) and GH are associated with low bone mineral density (BMD) and increased fracture risk. Replacement of T in hypogonadal men improves several bone parameters. Replacement of GH in GH-deficient men improves BMD.
Objective: Our objective was to determine whether T and GH treatment together improves the structural and mechanical parameters of bone more than T alone in men with hypopituitarism.
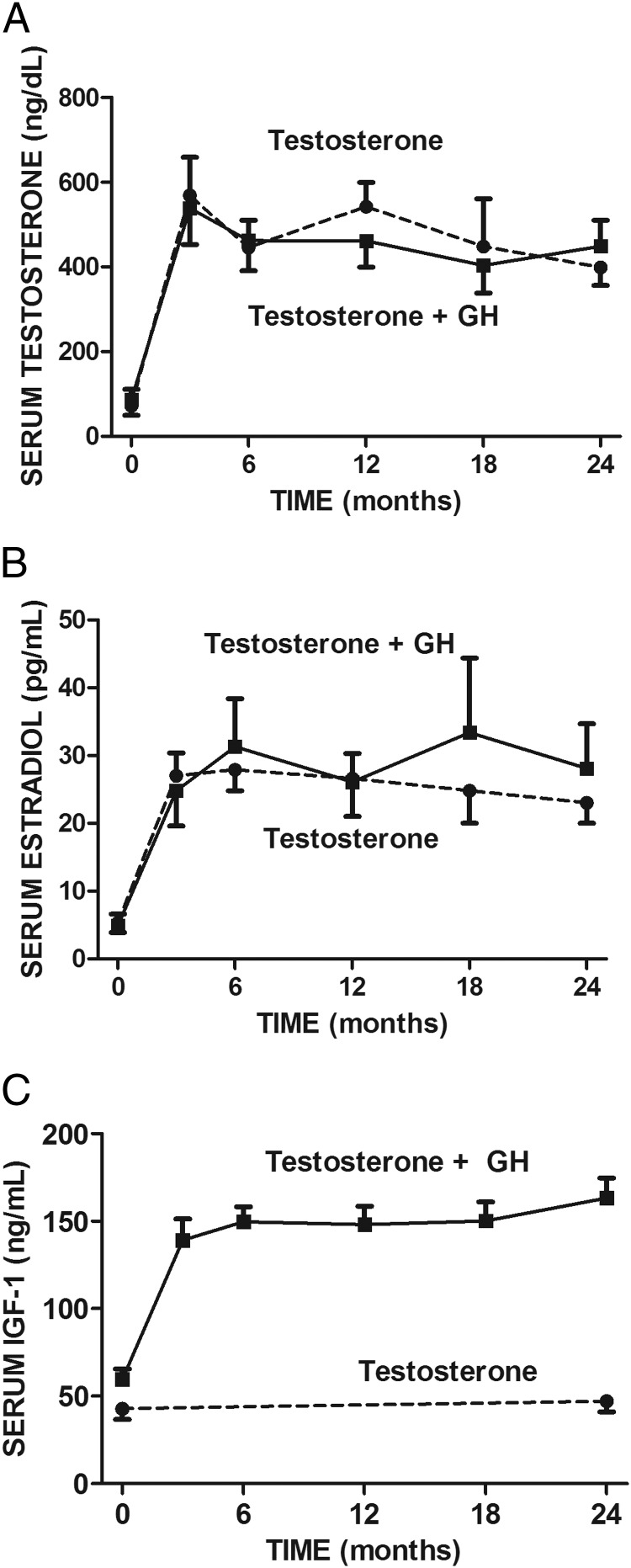
Design and subjects: This randomized, prospective, 2-year study included 32 men with severe deficiencies of T and GH due to panhypopituitarism.
Intervention: Subjects were randomized to receive T alone (n = 15) or T and GH (n = 17) for 2 years.
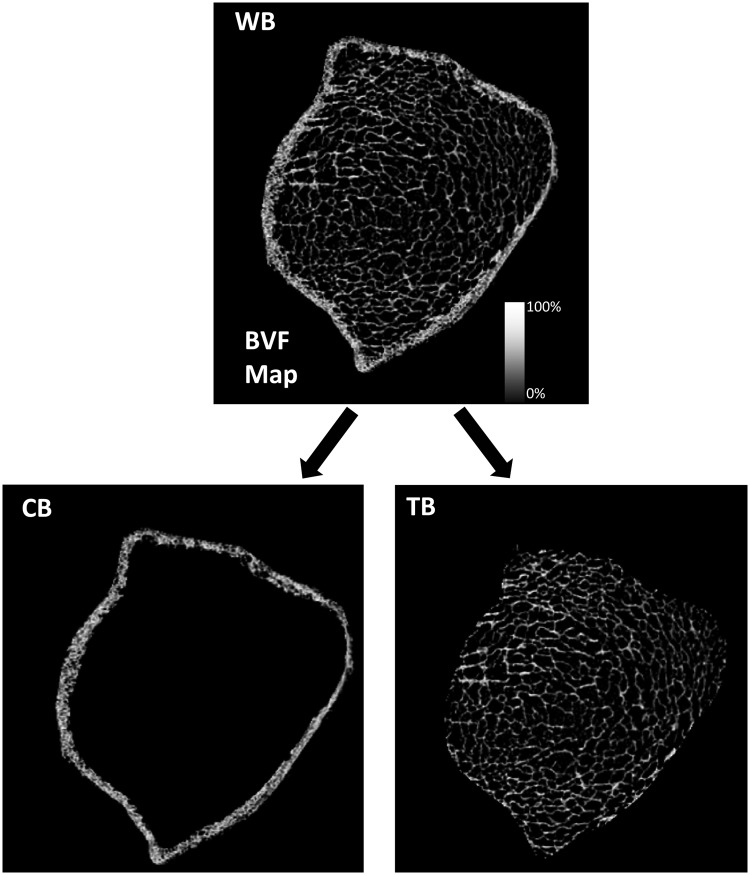
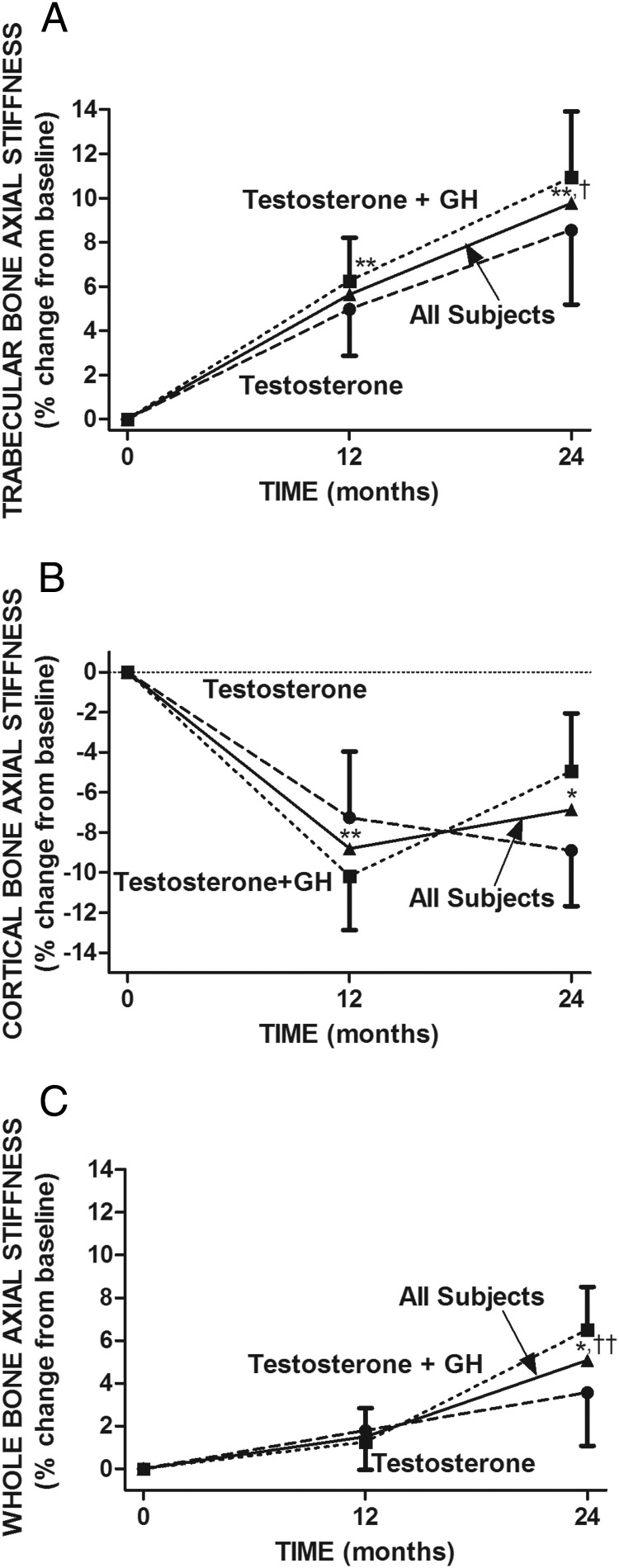
Main outcome measures: We evaluated magnetic resonance microimaging-derived structural (bone volume fraction [BVF] and trabecular thickness) and mechanical (axial stiffness [AS], a measure of bone strength) properties of the distal tibia at baseline and after 1 and 2 years of treatment.
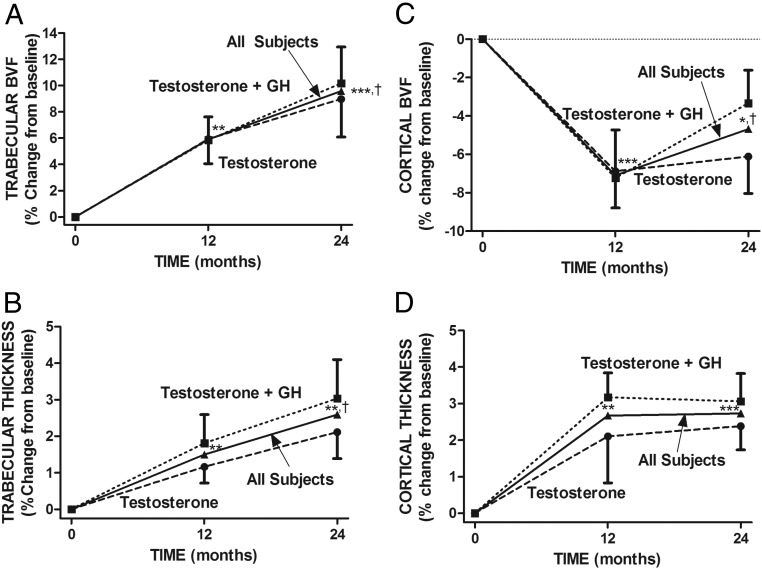
Results: Treatment with T and GH did not affect BVF, thickness, or AS differently from T alone. T treatment in all subjects for 2 years increased trabecular BVF by 9.6% (P < .0001), trabecular thickness by 2.6% (P < .001), and trabecular AS by 9.8% (P < .001). In contrast, testosterone treatment in all subjects significantly increased cortical thickness by 2.4% (P < .01) but decreased cortical BVF by -4.7% (P < .01) and cortical AS by -6.9% (P < .01).
Conclusion: Combined T and GH treatment of men with hypopituitarism for 2 years did not improve the measured structural or mechanical parameters of the distal tibia more than T alone. However, testosterone significantly increased the structural and mechanical properties of trabecular bone but decreased most of these properties of cortical bone, illustrating the potential importance of assessing trabecular and cortical bone separately in future studies of the effect of testosterone on bone.
Figures
References
-
- Greenspan SL, Coates P, Sereika SM, Nelson JB, Trump DL, Resnick NM. Bone loss after initiation of androgen deprivation therapy in patients with prostate cancer. J Clin Endocrinol Metab. 2005;90:6410–6417 - PubMed
-
- Stepán JJ, Lachman M, Zverina J, Pacovský V, Baylink DJ. Castrated men exhibit bone loss: effect of calcitonin treatment on biochemical indices of bone remodeling. J Clin Endocrinol Metab. 1989;69:523–527 - PubMed
-
- Wadhwa VK, Weston R, Mistry R, Parr NJ. Long-term changes in bone mineral density and predicted fracture risk in patients receiving androgen-deprivation therapy for prostate cancer, with stratification of treatment based on presenting values. BJU Int. 2009;104:800–805 - PubMed
-
- Hamilton EJ, Ghasem-Zadeh A, Gianatti E, et al. Structural decay of bone microarchitecture in men with prostate cancer treated with androgen deprivation therapy. J Clin Endocrinol Metab. 2010;95:E456–E463 - PubMed
-
- Benito M, Gomberg B, Wehrli FW, et al. Deterioration of trabecular architecture in hypogonadal men. J Clin Endocrinol Metab. 2003;88:1497–1502 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
