

Interventions to reduce rehospitalizations after chronic obstructive pulmonary disease exacerbations. A systematic review
- PMID: 24423379
- PMCID: PMC5467116
- DOI: 10.1513/AnnalsATS.201308-254OC
Interventions to reduce rehospitalizations after chronic obstructive pulmonary disease exacerbations. A systematic review
Abstract
Rationale: Approximately 20% of patients hospitalized for COPD exacerbations in the United States will be readmitted within 30 days. The Centers for Medicare and Medicaid Services has recently proposed to revise the Hospital Readmissions Reduction Program to financially penalize hospitals with high all-cause 30-day rehospitalization rates after a hospitalization for COPD exacerbation on or after October 1, 2014.
Objectives: To report the results of a systematic review of randomized clinical trials evaluating interventions to reduce the rehospitalizations after COPD exacerbations.
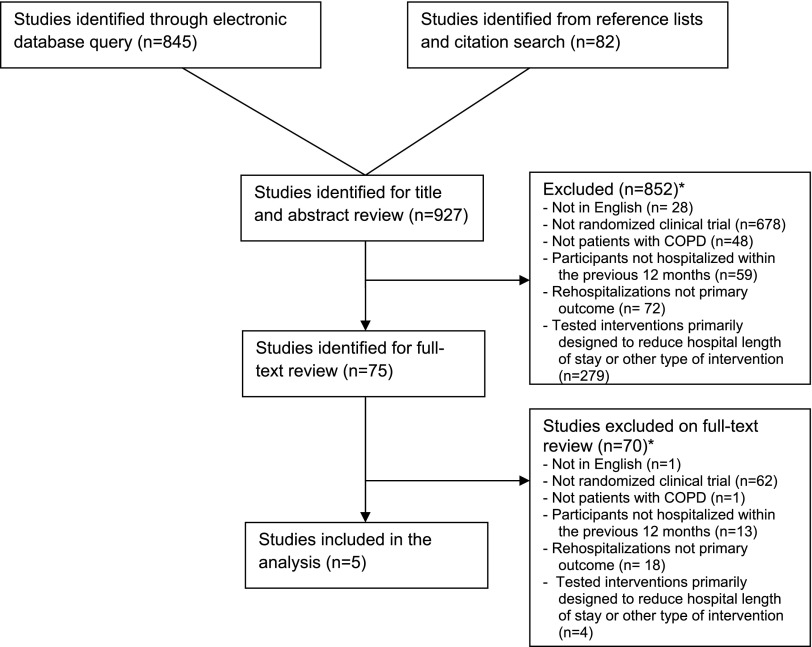
Methods: Multiple electronic databases were systematically searched to identify relevant studies published between January 1966 and June 2013. Titles, abstracts, and, subsequently, full-text articles were assessed for eligibility. Each study was appraised using predefined criteria.
Measurements and main results: Among 913 titles and abstracts screened, 5 studies (1,393 participants) met eligibility criteria. All studies had a primary outcome of rehospitalization at 6 or 12 months. No study examined 30-day rehospitalization as the primary outcome. Each study tested a different set of interventions. Two studies (one conducted in Canada and one conducted in Spain and Belgium) showed a decrease in all-cause rehospitalization over 12 months in the intervention group versus comparator group (mean number of hospitalizations per patient, 1.0 vs. 1.8; P = 0.01; percent hospitalized, 45 vs. 67%; P = 0.028; respectively). The only study conducted in the United States found a greater than twofold higher risk of mortality in the intervention group (17 vs. 7%, P = 0.003) but no significant difference in rehospitalizations. It was unclear which set of interventions was effective or harmful.
Conclusions: The evidence base is inadequate to recommend specific interventions to reduce rehospitalizations in this population and does not justify penalizing hospitals for high 30-day rehospitalization rates after COPD exacerbations.
Figures
References
-
- National Heart, Lung, and Blood Institute. Morbidity and mortality: 2009. chart book on cardiovascular, lung, and blood diseases [2011; accessed 2013 July12]. Available from: http://www.nhlbi.nih.gov/about/factbook/chapter4.htm
-
- Stein BD, Charbeneau JT, Lee TA, Schumock GT, Lindenauer PK, Bautista A, Lauderdale DS, Naureckas ET, Krishnan JA. Hospitalizations for acute exacerbations of chronic obstructive pulmonary disease: how you count matters. COPD. 2010;7:164–171. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- US CongressHouse Committee on Ways and Means, Committee on Energy and Commerce, Committee on Education and Labor. Compilation of Patient Protection and Affordable Care Act: As amended through 1 November 2010, including Patient Protection and Affordable Care Act health-related portions of the Health Care and Education Reconciliation Act of 2010. Washington, DC: U.S. Government Printing Office; 2010. xxiii
-
- Department of Health and Human ServicesCenters for Medicare and Medicaid Services. Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long- Term Care Hospital Prospective Payment System and Proposed Fiscal Year 2014 Rates; Quality Reporting Requirements for Specific Providers; Hospital Conditions of Participation [Internet]. National Archives and Records Administration; 2013. May [accessed 2013 July 14]. 78 Federal Register 91. Available from: http://www.gpo.gov/fdsys/pkg/FR-2013-05-10/pdf/2013-10234.pdf - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
