

Site-specific antibody drug conjugates for cancer therapy
- PMID: 24423619
- PMCID: PMC3929453
- DOI: 10.4161/mabs.27022
Site-specific antibody drug conjugates for cancer therapy
Abstract
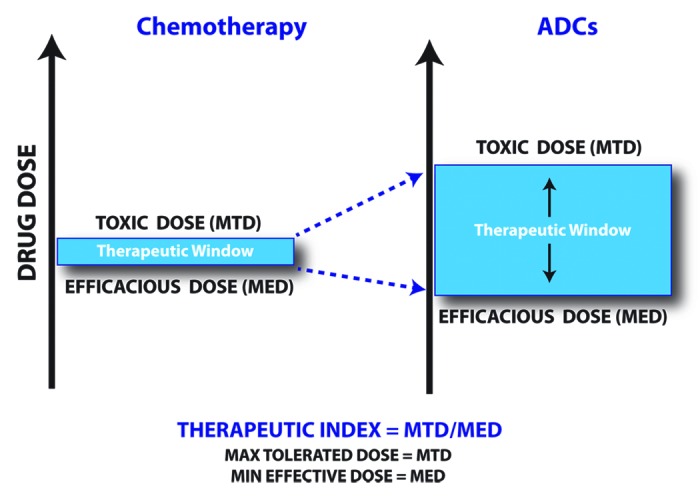
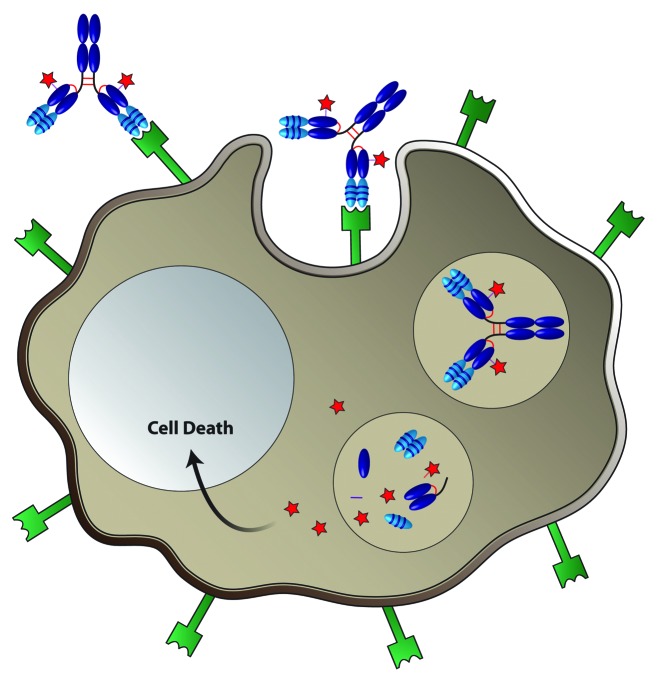
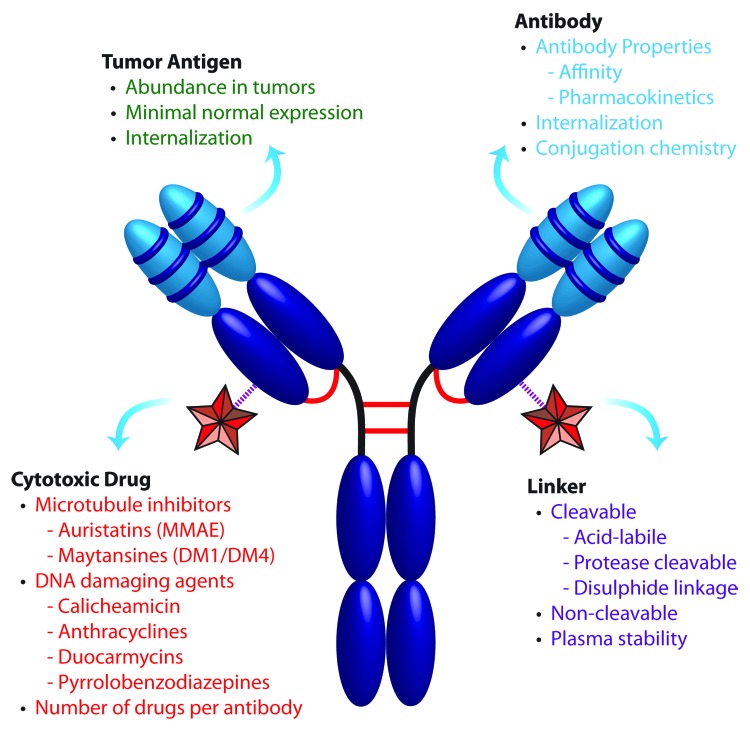
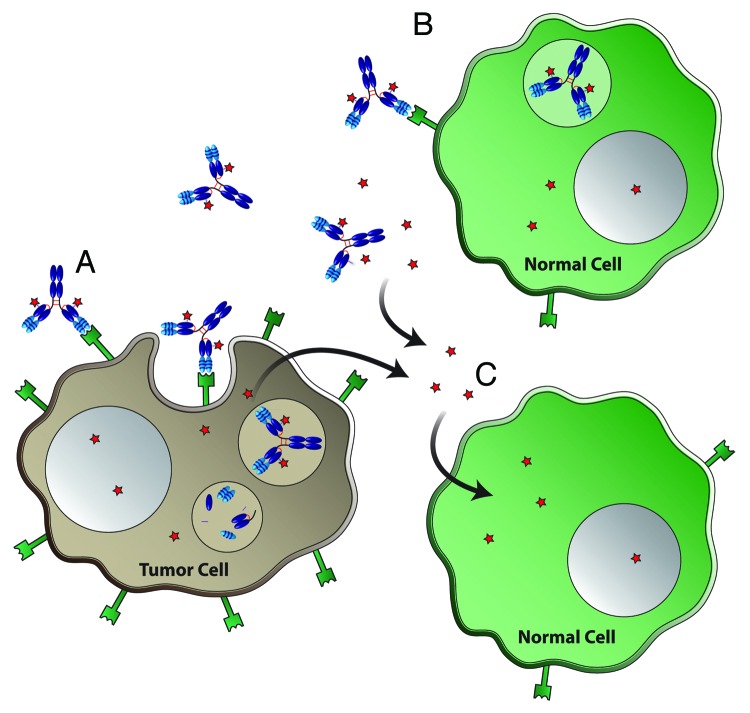
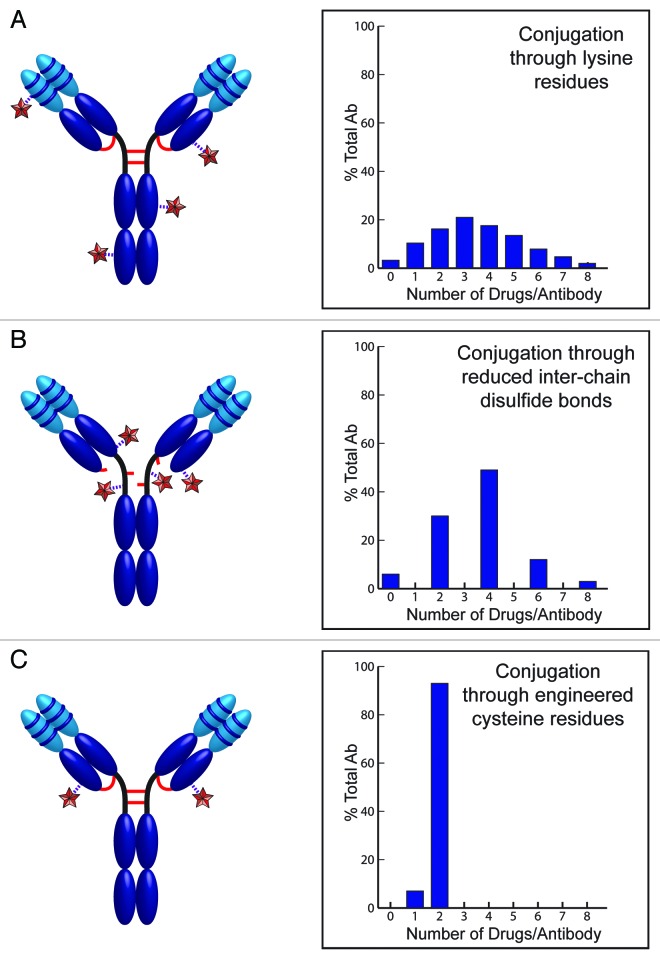
Antibody therapeutics have revolutionized the treatment of cancer over the past two decades. Antibodies that specifically bind tumor surface antigens can be effective therapeutics; however, many unmodified antibodies lack therapeutic activity. These antibodies can instead be applied successfully as guided missiles to deliver potent cytotoxic drugs in the form of antibody drug conjugates (ADCs). The success of ADCs is dependent on four factors--target antigen, antibody, linker, and payload. The field has made great progress in these areas, marked by the recent approval by the US Food and Drug Administration of two ADCs, brentuximab vedotin (Adcetris) and ado-trastuzumab emtansine (Kadcyla). However, the therapeutic window for many ADCs that are currently in pre-clinical or clinical development remains narrow and further improvements may be required to enhance the therapeutic potential of these ADCs. Production of ADCs is an area where improvement is needed because current methods yield heterogeneous mixtures that may include 0-8 drug species per antibody molecule. Site-specific conjugation has been recently shown to eliminate heterogeneity, improve conjugate stability, and increase the therapeutic window. Here, we review and describe various site-specific conjugation strategies that are currently used for the production of ADCs, including use of engineered cysteine residues, unnatural amino acids, and enzymatic conjugation through glycotransferases and transglutaminases. In addition, we also summarize differences among these methods and highlight critical considerations when building next-generation ADC therapeutics.
Keywords: THIOMAB; antibody drug conjugate; cytotoxic drug; internalization; linker; site-specific conjugation; tumor antigen.
Figures
References
-
- Shuptrine CW, Surana R, Weiner LM. . Monoclonal antibodies for the treatment of cancer. Semin Cancer Biol 2012; 22:3 - 13; http://dx.doi.org/ 10.1016/j.semcancer.2011.12.009; PMID: 22245472 - DOI - PMC - PubMed
-
- Reichert JM, Rosensweig CJ, Faden LB, Dewitz MC. . Monoclonal antibody successes in the clinic. Nat Biotechnol 2005; 23:1073 - 8; http://dx.doi.org/ 10.1038/nbt0905-1073; PMID: 16151394 - DOI - PubMed
-
- Kubota T, Niwa R, Satoh M, Akinaga S, Shitara K, Hanai N. . Engineered therapeutic antibodies with improved effector functions. Cancer Sci 2009; 100:1566 - 72; http://dx.doi.org/ 10.1111/j.1349-7006.2009.01222.x; PMID: 19538497 - DOI - PMC - PubMed
-
- Lambert JM. . Drug-conjugated monoclonal antibodies for the treatment of cancer. Curr Opin Pharmacol 2005; 5:543 - 9; http://dx.doi.org/ 10.1016/j.coph.2005.04.017; PMID: 16087399 - DOI - PubMed
-
- Senter PD. . Potent antibody drug conjugates for cancer therapy. Curr Opin Chem Biol 2009; 13:235 - 44; http://dx.doi.org/ 10.1016/j.cbpa.2009.03.023; PMID: 19414278 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous