

Lower mitotic activity in BRCA1/2-associated primary breast cancers occurring after risk-reducing salpingo-oophorectomy
- PMID: 24423863
- PMCID: PMC3979814
- DOI: 10.4161/cbt.27628
Lower mitotic activity in BRCA1/2-associated primary breast cancers occurring after risk-reducing salpingo-oophorectomy
Abstract
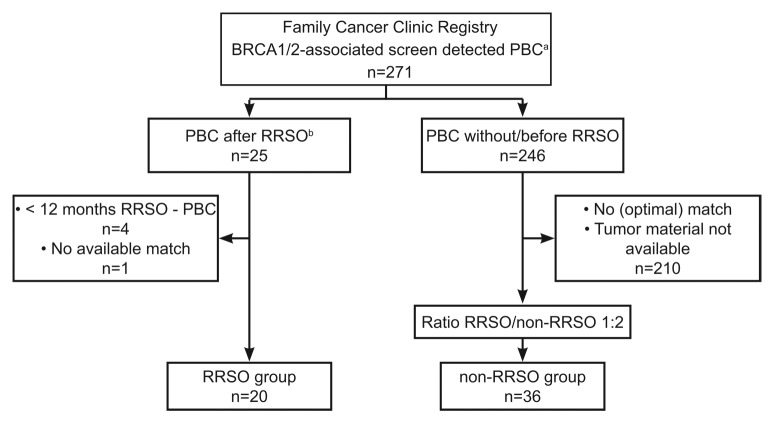
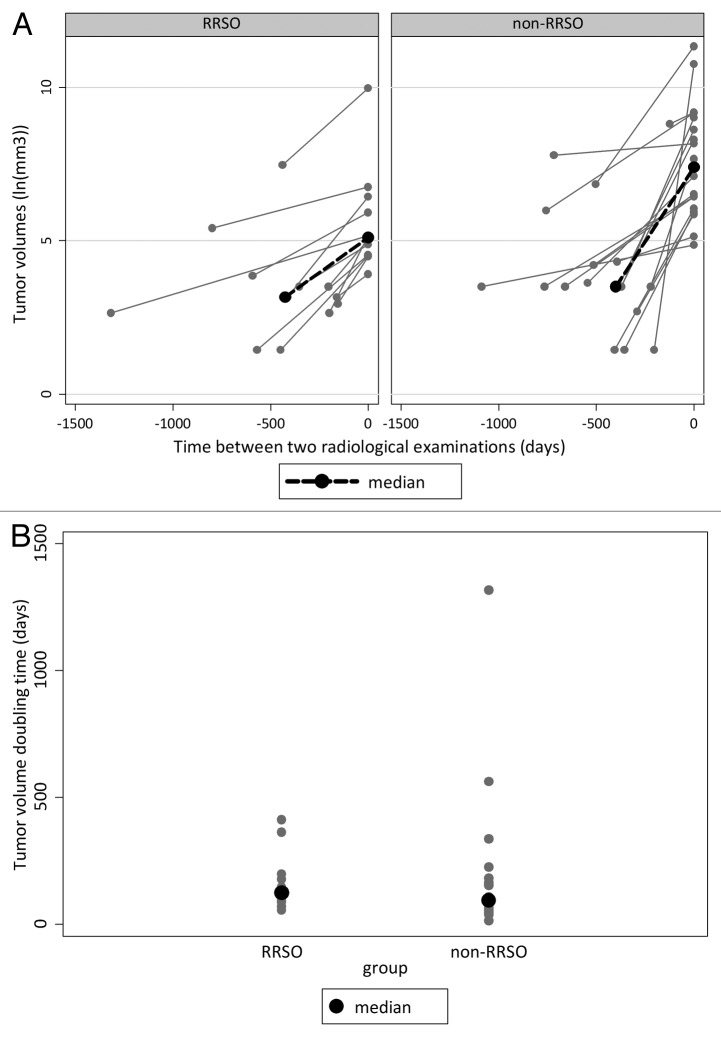
Risk-reducing salpingo-oophorectomy (RRSO) is associated with 50% reduction of BRCA1/2-associated breast cancer (BC) risk, possibly through decreased growth activity. In this pilot study, tumor characteristics and growth rates of BRCA1/2-associated primary BCs (PBCs) detected after RRSO were compared with those of PBCs originating without RRSO. From a cohort of 271 women with BRCA1/2-associated screen detected BC, we selected 20 patients with PBC detected ≥12 months after RRSO (RRSO group). Controls were 36 BRCA1/2 mutation carriers with PBC detected without RRSO (non-RRSO group) matched for age at diagnosis (± 2.5 y) and for BRCA1 or BRCA2 mutation. Pathology samples were revised for histological subtype, tumor differentiation grade, mitotic activity index (MAI), estrogen receptor (ER), progesterone receptor (PR), and HER2 status. Tumor growth rates, expressed as tumor volume doubling times (DT), were calculated from revised magnetic resonance and mammographic images. Median age at PBC diagnosis was 52 y (range 35-67). PBCs after RRSO had lower MAIs (12 vs. 22 mitotic counts/2 mm, P = 0.02), were smaller (11 vs. 17 mm, P = 0.01), and tend to be PR-positive more often than PBCs without RRSO (38% vs. 13%, P = 0.07). Differentiation grade, ER, and HER2 status were not different. Median DT was 124 d (range 89-193) in the RRSO group and 93 days (range 54-253) in the non-RRSO group (P = 0.47). BC occurring after RRSO in BRCA mutation carriers features a lower MAI, suggesting a less aggressive biological phenotype. When confirmed in larger series, this may have consequences for BC screening protocols after RRSO.
Keywords: BRCA1/2; breast cancer; estrogen; mitotic activity; risk-reducing salpingo-oophorectomy; tumor characteristics; tumor growth.
Figures
References
-
- van der Kolk DM, de Bock GH, Leegte BK, Schaapveld M, Mourits MJ, de Vries J, van der Hout AH, Oosterwijk JC. Penetrance of breast cancer, ovarian cancer and contralateral breast cancer in BRCA1 and BRCA2 families: high cancer incidence at older age. Breast Cancer Res Treat. 2010;124:643–51. doi: 10.1007/s10549-010-0805-3. - DOI - PubMed
-
- Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72:1117–30. doi: 10.1086/375033. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous