

Review
doi: 10.1210/er.2013-1029.
Epub 2013 Dec 20.
Adrenocortical carcinoma
Affiliations
- PMID: 24423978
- PMCID: PMC3963263
- DOI: 10.1210/er.2013-1029
Item in Clipboard
Review
Adrenocortical carcinoma
Endocr Rev.
2014 Apr.
Abstract
Adrenocortical carcinoma (ACC) is a rare endocrine malignancy, often with an unfavorable prognosis. Here we summarize the knowledge about diagnosis, epidemiology, pathophysiology, and therapy of ACC. Over recent years, multidisciplinary clinics have formed and the first international treatment trials have been conducted. This review focuses on evidence gained from recent basic science and clinical research and provides perspectives from the experience of a large multidisciplinary clinic dedicated to the care of patients with ACC.
Figures
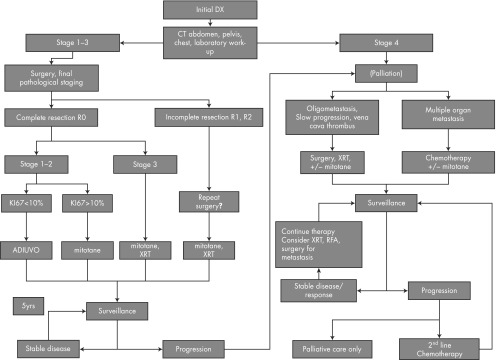
Flow chart for ACC therapy. Abbreviations: Dx, diagnosis; XRT, radiation therapy.
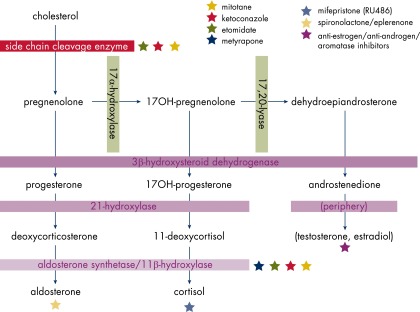
Steroidogenesis and inhibitors.
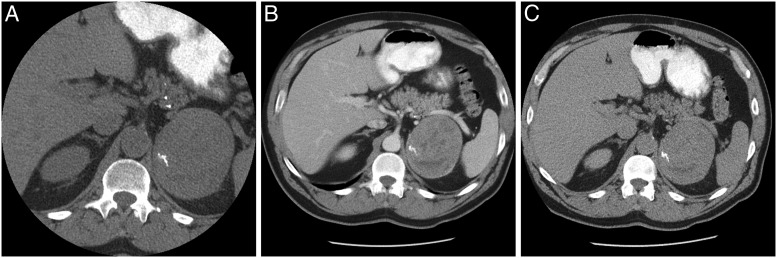
ACC. A, Precontrast fairly homogeneous with calcification (30 HU). B, Early-phase contrast with heterogeneous enhancement. C, Delayed phase (15 minutes).
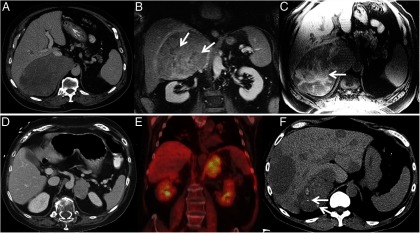
A, CT of ACC showing large heterogeneous right adrenal tumor, B, Contrast-enhanced coronal MRI in the same patient showing heterogeneous enhancement with nonenhancing areas of necrosis (arrows). C, Non–contrast-enhanced T1-weighted MRI in the same patient showing T1-weighted hyperintense areas of hemorrhage (arrows). D, CT of ACC showing left adrenal tumor. E, Intensely FDG avid left adrenal mass in the same patient. F, Metastasized ACC, calcifications in primary tumor (arrows).
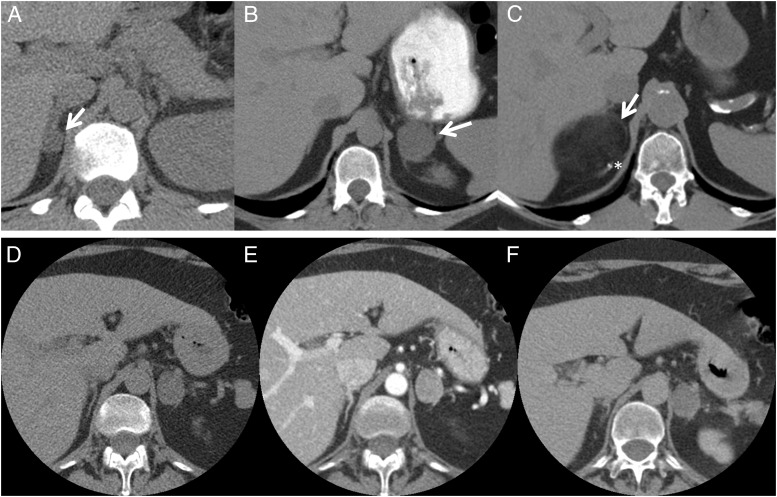
A, Small right adrenal adenoma with <10 HU on unenhanced CT scan. B, Left adrenal adenoma with <10 HU on unenhanced CT scan. C, Myelolipoma with fat attenuation and small calcification (asterisk). D–F, Dedicated adrenal CT scan without contrast, 16 HU (D); immediately after contrast, 99 HU (E); and delayed image, 44 HU (F), identifying this lesion as a non–lipid-rich adenoma.
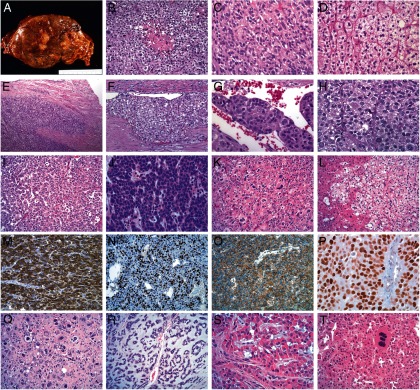
A, ACC gross. Adrenocortical tumors tend to be relatively large masses (>5 cm in largest diameter) that grow by expansion. Their cut surface ranges from brown to orange to yellow depending on the lipid content of their cells. Necrosis is almost always present. B, Typical ACC with a hypercellular population of cells with the earliest form of tumor necrosis. C, A typical ACC with a solid growth pattern and abundant eosinophilic cytoplasm with focal clear areas, consistent with lipid. Mitotic figures are present. D, A lipid-rich ACA with nested growth pattern and clear cytoplasm is shown for comparison with ACC. E, Direct invasion of the tumor capsule, representing the earliest manifestation of malignant behavior. F, Relatively differentiated ACC that has invaded a vessel within the tumor capsule. G, ACC tumor thrombus covered with endothelial cells. H, High-grade ACC with high nuclear grade, diffuse growth pattern, eosinophilic cytoplasm, and 3 visible mitotic figures. I, Low-grade ACC with abundant cytoplasm and low mitotic rate. J, High-grade ACC with minimal cytoplasm, resembling small cell carcinoma. K, Low-grade ACC with isolated nuclear pleomorphism. L, ACC metastatic to liver. Notice the lipid-rich nature of the tumor and the lack of stromal response. M, α-Inhibin immunohistochemistry showing diffuse immunoreactivity in ACC. N, Ki67 immunohistochemistry showing a high labeling index in a high-grade ACC. O, β-Catenin immunohistochemistry showing pure membranous staining in ACC, indicating a wild-type CTNNB1 gene. P, p53 immunohistochemistry showing diffuse immunoreactivity in a high-grade ACC, indicating a likely somatic TP53 mutation. Q, Postchemotherapy effect in ACC, showing large cells with bizarre nuclear forms. R, Myxoid variant of ACC with abundant extracellular myxoid material. S, Rare oncocytic variant of ACC that also has focal myxoid stroma. T, Adrenocortical oncocytoma with isolated multinucleated cells.
References
-
- Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004;25:309–340 - PubMed
-
- Viani GA, Stefano EJ, Afonso SL. Higher-than-conventional radiation doses in localized prostate cancer treatment: a meta-analysis of randomized, controlled trials. Int J Radiat Oncol Biol Phys. 2009;74:1405–1418 - PubMed
-
- Allolio B, Fassnacht M. Clinical review: Adrenocortical carcinoma: clinical update. J Clin Endocrinol Metab. 2006;91:2027–2037 - PubMed
-
- Kebebew E, Reiff E, Duh QY, Clark OH, McMillan A. Extent of disease at presentation and outcome for adrenocortical carcinoma: have we made progress? World J Surg. 2006;30:872–878 - PubMed
-
- Pianovski MA, Maluf EM, de Carvalho DS, et al. Mortality rate of adrenocortical tumors in children under 15 years of age in Curitiba, Brazil. Pediatr Blood Cancer. 2006;47:56–60 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
