

Interpreting treatment effects from clinical trials in the context of real-world risk information: end-stage renal disease prevention in older adults
- PMID: 24424348
- PMCID: PMC4119007
- DOI: 10.1001/jamainternmed.2013.13328
Interpreting treatment effects from clinical trials in the context of real-world risk information: end-stage renal disease prevention in older adults
Abstract
Importance: Older adults are often excluded from clinical trials. The benefit of preventive interventions tested in younger trial populations may be reduced when applied to older adults in the clinical setting if they are less likely to survive long enough to experience those outcomes targeted by the intervention.
Objective: To extrapolate a treatment effect similar to those reported in major randomized clinical trials of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for prevention of end-stage renal disease (ESRD) to a real-world population of older patients with chronic kidney disease.
Design, setting, and participants: Simulation study in a retrospective cohort conducted in Department of Veterans Affairs medical centers. We included 371 470 patients 70 years or older with chronic kidney disease.
Exposure: Level of estimated glomerular filtration rate (eGFR) and proteinuria.
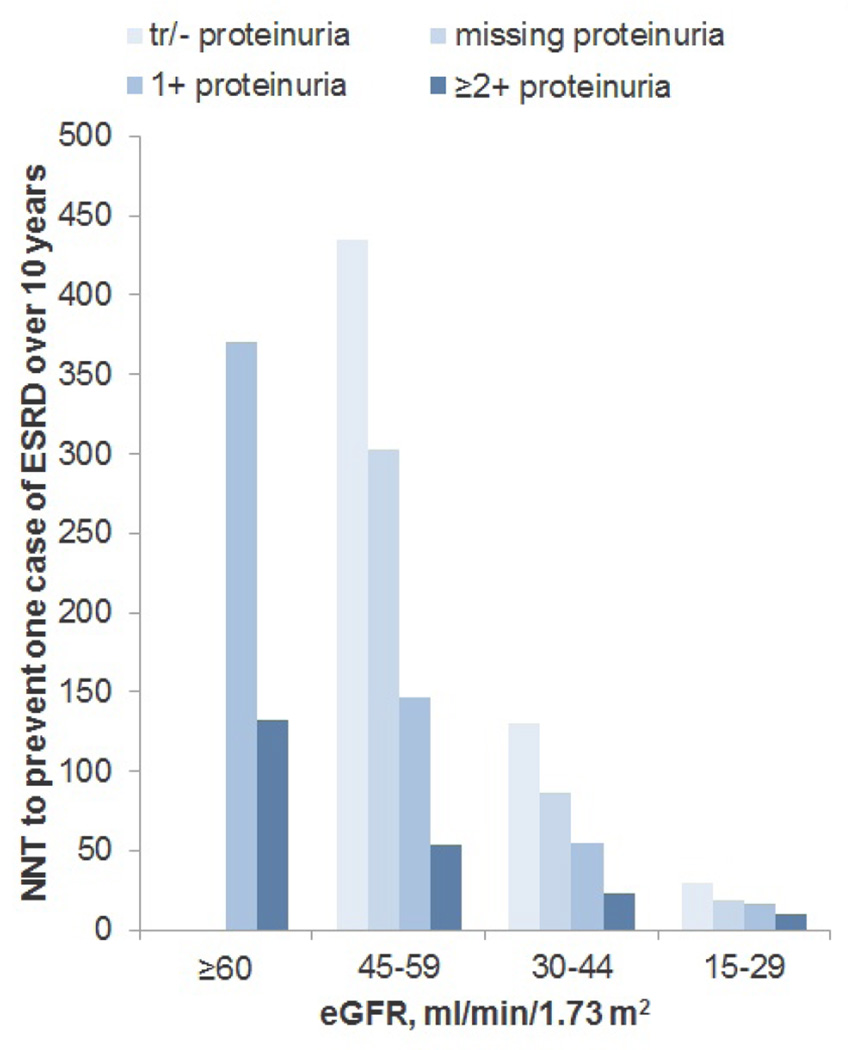
Main outcomes and measures: Among members of this cohort, we evaluated the expected effect of a 30% reduction in relative risk on the number needed to treat (NNT) to prevent 1 case of ESRD over a 3-year period. These limits were selected to mimic the treatment effect achieved in major trials of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for prevention of ESRD. These trials have reported relative risk reductions of 23% to 56% during observation periods of 2.6 to 3.4 years, yielding NNTs to prevent 1 case of ESRD of 9 to 25.
Results: The NNT to prevent 1 case of ESRD among members of this cohort ranged from 16 in patients with the highest baseline risk (eGFR of 15-29 mL/min/1.73 m(2) with a dipstick proteinuria measurement of ≥ 2+) to 2500 for those with the lowest baseline risk (eGFR of 45-59 mL/min/1.73 m(2) with negative or trace proteinuria and eGFR of ≥ 60 mL/min/1.73 m2 with dipstick proteinuria measurement of 1+). Most patients belonged to groups with an NNT of more than 100, even when the exposure time was extended over 10 years and in all sensitivity analyses.
Conclusions and relevance: Differences in baseline risk and life expectancy between trial subjects and real-world populations of older adults with CKD may reduce the marginal benefit to individual patients of interventions to prevent ESRD.
Figures
Comment in
-
The gap between clinical trials and the real world: extrapolating treatment effects from younger to older adults.JAMA Intern Med. 2014 Mar;174(3):397-8. doi: 10.1001/jamainternmed.2013.13283. JAMA Intern Med. 2014. PMID: 24424303 No abstract available.
References
-
- Van Spall HG, Toren A, Kiss A, Fowler RA. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: a systematic sampling review. JAMA. 2007;297(11):1233–1240. - PubMed
-
- Lee PY, Alexander KP, Hammill BG, Pasquali SK, Peterson ED. Representation of elderly persons and women in published randomized trials of acute coronary syndromes. JAMA. 2001;286(6):708–713. - PubMed
-
- Gurwitz JH, Col NF, Avorn J. The exclusion of the elderly and women from clinical trials in acute myocardial infarction. JAMA. 1992;268(11):1417–1422. - PubMed
-
- Heiat A, Gross CP, Krumholz HM. Representation of the elderly, women, and minorities in heart failure clinical trials. Arch Intern Med. 2002;162(15):1682–1688. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
