

A comparative review of escitalopram, paroxetine, and sertraline: Are they all alike?
- PMID: 24424469
- PMCID: PMC4047306
- DOI: 10.1097/YIC.0000000000000023
A comparative review of escitalopram, paroxetine, and sertraline: Are they all alike?
Abstract
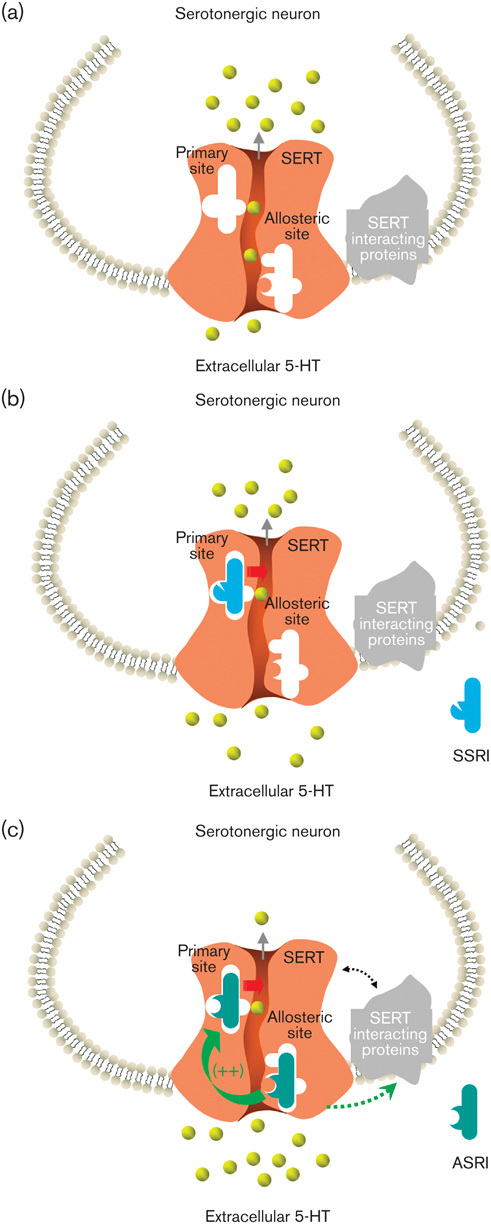
It is known that newer antidepressants, such as the selective serotonin reuptake inhibitors (SSRIs), provide advantages in tolerability over antidepressants such as the tricyclics. However, even within the SSRI class, differences in efficacy or tolerability exist between the individual drugs. Among the three most widely prescribed SSRIs are paroxetine, sertraline, and escitalopram. Escitalopram is commonly referred to as an SSRI, but also has well-documented allosteric properties, and thus can be further classed as an allosteric serotonin reuptake inhibitor. All three antidepressants are efficacious compared with placebo, but there is evidence that escitalopram is more effective than a range of other antidepressants. There are no direct data to regard either paroxetine or sertraline as a superior antidepressant. Escitalopram is superior compared with paroxetine, which has a less favorable tolerability profile. Paroxetine is associated with cholinergic muscarinic antagonism and potent inhibition of CYP2D6, and sertraline has moderate drug interaction issues in comparison with escitalopram. Overall, as an allosteric serotonin reuptake inhibitor that is somewhat different from classical SSRIs, escitalopram is the first choice judged by combined efficacy and tolerability, and nonclinical data have offered possible mechanisms through which escitalopram could be more efficacious, based on its interaction with orthosteric and allosteric binding sites at the serotonin transporter.
Figures
References
-
- Aberg-Wistedt A, Agren H, Ekselius L, Bengtsson F, Akerblad AC.Sertraline versus paroxetine in major depression: clinical outcome after six months of continuous therapy.J Clin Psychopharmacol 2000;20:645–652 - PubMed
-
- Alexopoulos G, Gordon J, Zhang D.A placebo-controlled trial of escitalopram and sertraline in the treatment of major depressive disorder.Neuropsychopharmacology 2004;29SupplS87
-
- Arnt J, Christensen AV, Hyttel J.Pharmacology in vivo of the phenylindan derivative, Lu 19-005, a new potent inhibitor of dopamine, noradrenaline and 5-hydroxytryptamine uptake in rat brain.Naunyn Schmiedebergs Arch Pharmacol 1985;329:101–107 - PubMed
-
- Baldwin DS, Cooper JA, Huusom AK, Hindmarch I.A double-blind, randomized, parallel-group, flexible-dose study to evaluate the tolerability, efficacy and effects of treatment discontinuation with escitalopram and paroxetine in patients with major depressive disorder.Int Clin Psychopharmacol 2006;21:159–169 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
