

AR function in promoting metastatic prostate cancer
- PMID: 24425228
- PMCID: PMC4452946
- DOI: 10.1007/s10555-013-9471-3
AR function in promoting metastatic prostate cancer
Abstract
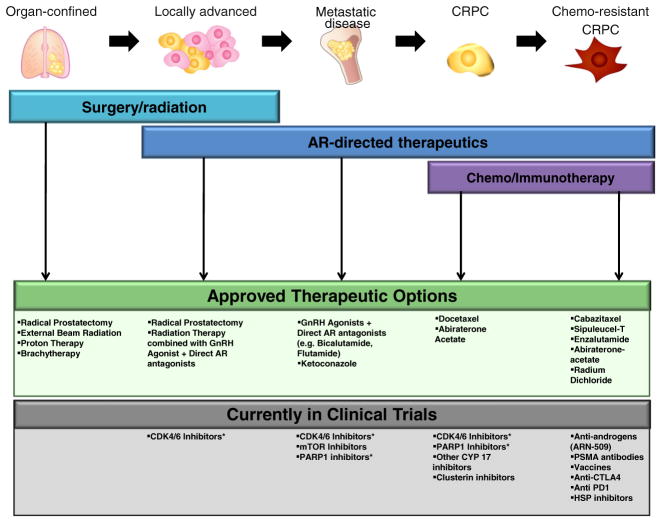
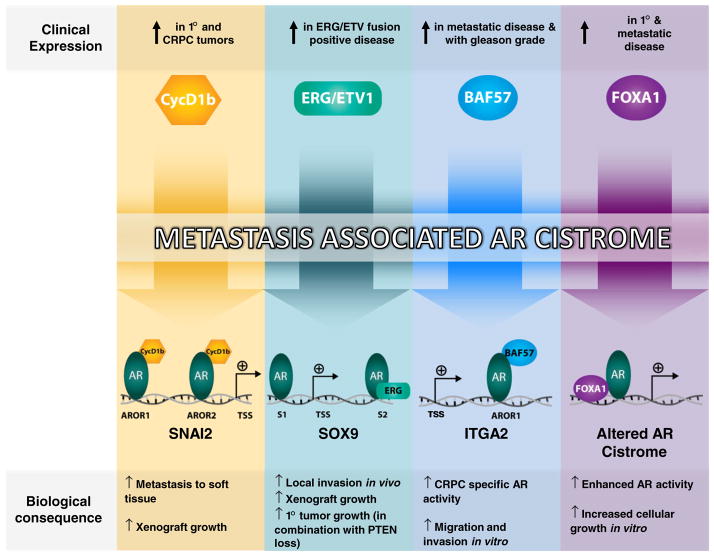
Prostate cancer (PCa) remains a leading cause of cancer-related death in the USA. While localized lesions are effectively treated through radical prostatectomy and/or radiation therapy, treatment for metastatic disease leverages the addiction of these tumors on the androgen receptor (AR) signaling axis for growth and disease progression. Though initially effective, tumors resistant to AR-directed therapeutics ultimately arise (a stage of the disease known as castration-resistant prostate cancer) and are responsible for PCa-specific mortality. Importantly, an abundance of clinical and preclinical evidence strongly implicates AR signaling cascades in the development of metastatic disease in both early and late stages, and thus a concerted effort has been made to delineate the AR-specific programs that facilitate progression to metastatic PCa. A multitude of downstream AR targets as well as critical AR cofactors have been identified which impinge upon both the AR pathway as well as associated metastatic phenotypes. This review will highlight the functional significance of these pathways to disseminated disease and define the molecular underpinnings behind these unique, AR-driven, metastatic signatures.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics. CA A Cancer Journal for Clinicians. 2012;62:10–29. - PubMed
-
- Klein EA, Ciezki J, Kupelian PA, Mahadevan A. Outcomes for intermediate risk prostate cancer: are there advantages for surgery, external radiation, or brachytherapy? Urologic Oncology. 2009;27:67–71. - PubMed
-
- Klotz L. Combined androgen blockade: an update. The Urologic Clinics of North America. 2006;33:161–166. v–vi. - PubMed
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. Journal of Clinical Oncology. 2007;25:1596–1605. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
