

Who needs laboratories and who needs statins?: comparative and cost-effectiveness analyses of non-laboratory-based, laboratory-based, and staged primary cardiovascular disease screening guidelines
- PMID: 24425701
- PMCID: PMC3971865
- DOI: 10.1161/CIRCOUTCOMES.113.000397
Who needs laboratories and who needs statins?: comparative and cost-effectiveness analyses of non-laboratory-based, laboratory-based, and staged primary cardiovascular disease screening guidelines
Abstract
Background: Early detection and treatment of cardiovascular disease (CVD) risk factors produces significant clinical benefits, but no consensus exists on optimal screening algorithms. This study aimed to evaluate the comparative and cost-effectiveness of staged laboratory-based and non-laboratory-based total CVD risk assessment.
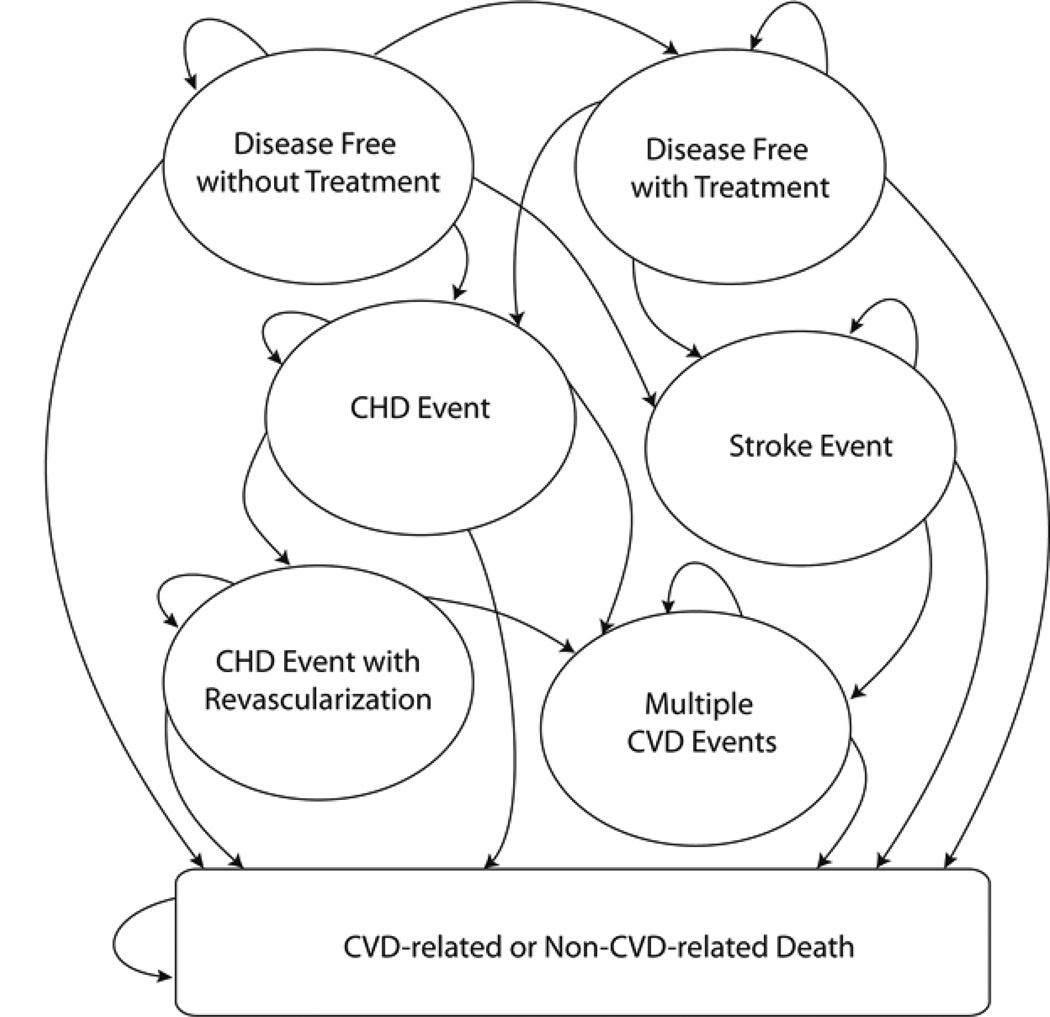
Methods and results: We used receiver operating characteristic curve and cost-effectiveness modeling methods to compare strategies with and without laboratory components and used single-stage and multistage algorithms, including approaches based on Framingham risk scores (laboratory-based assessments for all individuals). Analyses were conducted using data from 5998 adults in the Third National Health and Nutrition Examination Survey without history of CVD using 10-year CVD death as the main outcome. A microsimulation model projected lifetime costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios for 60 Framingham-based, non-laboratory-based, and staged screening approaches. Across strategies, the area under the receiver operating characteristic curve was 0.774 to 0.780 in men and 0.812 to 0.834 in women. There were no statistically significant differences in area under the receiver operating characteristic curve between multistage and Framingham-based approaches. In cost-effectiveness analyses, multistage strategies had incremental cost-effectiveness ratios of $52,000/QALY and $83,000/QALY for men and women, respectively. Single-stage/Framingham-based strategies were dominated (higher cost and lower QALYs) or had unattractive incremental cost-effectiveness ratios (>$300,000/QALY) compared with single-stage/non-laboratory-based and multistage approaches.
Conclusions: Non-laboratory-based CVD risk assessment can be useful in primary CVD prevention as a substitute for laboratory-based assessments or as the initial component of a multistage approach. Cost-effective multistage screening strategies could avoid 25% to 75% of laboratory testing used in CVD risk screening with predictive power comparable with Framingham risks.
Keywords: diagnosis; economics; primary prevention.
Conflict of interest statement
Figures



Similar articles
-
Cost-effectiveness of the polypill versus risk assessment for prevention of cardiovascular disease.Heart. 2017 Apr;103(7):483-491. doi: 10.1136/heartjnl-2016-310529. Epub 2017 Jan 11. Heart. 2017. PMID: 28077465
-
Results of a Markov model analysis to assess the cost-effectiveness of statin therapy for the primary prevention of cardiovascular disease in Korea: the Korean Individual-Microsimulation Model for Cardiovascular Health Interventions.Clin Ther. 2009 Dec;31(12):2919-30; discussion 2916-8. doi: 10.1016/j.clinthera.2009.12.013. Clin Ther. 2009. PMID: 20110032
-
Lifetime effects and cost-effectiveness of statin therapy for older people in the United Kingdom: a modelling study.Heart. 2024 Oct 10;110(21):1277-1285. doi: 10.1136/heartjnl-2024-324052. Heart. 2024. PMID: 39256053 Free PMC article.
-
Modeling the costs and long-term health benefits of screening the general population for risks of cardiovascular disease: a review of methods used in the literature.Eur J Health Econ. 2016 Nov;17(8):1041-1053. doi: 10.1007/s10198-015-0753-2. Epub 2015 Dec 18. Eur J Health Econ. 2016. PMID: 26682549 Free PMC article. Review.
-
Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis.Lancet. 2006 Aug 19;368(9536):679-86. doi: 10.1016/S0140-6736(06)69252-0. Lancet. 2006. PMID: 16920473 Free PMC article. Review.
Cited by
-
[Effectiveness of statin treatment strategies for primary prevention of cardiovascular diseases in a community-based Chinese population: A decision-analytic Markov model].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Jun 18;54(3):443-449. doi: 10.19723/j.issn.1671-167X.2022.03.008. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35701120 Free PMC article. Chinese.
-
Cost-effectiveness of implementing risk-based cardiovascular disease (CVD) management using updated WHO CVD risk prediction charts in India.PLoS One. 2023 Aug 25;18(8):e0285542. doi: 10.1371/journal.pone.0285542. eCollection 2023. PLoS One. 2023. PMID: 37624838 Free PMC article.
-
An assessment of community health workers' ability to screen for cardiovascular disease risk with a simple, non-invasive risk assessment instrument in Bangladesh, Guatemala, Mexico, and South Africa: an observational study.Lancet Glob Health. 2015 Sep;3(9):e556-63. doi: 10.1016/S2214-109X(15)00143-6. Epub 2015 Jul 14. Lancet Glob Health. 2015. PMID: 26187361 Free PMC article.
-
Cost-effectiveness of 10-Year Risk Thresholds for Initiation of Statin Therapy for Primary Prevention of Cardiovascular Disease.JAMA. 2015 Jul 14;314(2):142-50. doi: 10.1001/jama.2015.6822. JAMA. 2015. PMID: 26172894 Free PMC article.
-
Health Impact and Cost-Effectiveness of Achieving the National Salt and Sugar Reduction Initiative Voluntary Sugar Reduction Targets in the United States: A Microsimulation Study.Circulation. 2021 Oct 26;144(17):1362-1376. doi: 10.1161/CIRCULATIONAHA.121.053678. Epub 2021 Aug 27. Circulation. 2021. PMID: 34445886 Free PMC article.
References
-
- Mosca L. Guidelines for prevention of cardiovascular disease in women: A summary of recommendations. Prev Cardiol. 2007;10(Suppl 4):19–25. - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, Dallongeville J, De Backer G, Ebrahim S, Gjelsvik B, Herrmann-Lingen C, Hoes A, Humphries S, Knapton M, Perk J, Priori SG, Pyorala K, Reiner Z, Ruilope L, Sans-Menendez S, Op Reimer WS, Weissberg P, Wood D, Yarnell J, Zamorano JL, Walma E, Fitzgerald T, Cooney MT, Dudina A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Funck-Brentano C, Filippatos G, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Altiner A, Bonora E, Durrington PN, Fagard R, Giampaoli S, Hemingway H, Hakansson J, Kjeldsen SE, Larsen L, Mancia G, Manolis AJ, Orth-Gomer K, Pedersen T, Rayner M, Ryden L, Sammut M, Schneiderman N, Stalenhoef AF, Tokgozoglu L, Wiklund O, Zampelas A. European guidelines on cardiovascular disease prevention in clinical practice: Full text. Fourth joint task force of the european society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts) Eur J Cardiovasc Prev Rehabil. 2007;14(Suppl 2):S1–S113. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
