

Massive Liver Trauma-Multidisciplinary Approach and Minimal Invasive Surgery can Salvage Patients
- PMID: 24426645
- PMCID: PMC3693273
- DOI: 10.1007/s12262-012-0781-4
Massive Liver Trauma-Multidisciplinary Approach and Minimal Invasive Surgery can Salvage Patients
Abstract
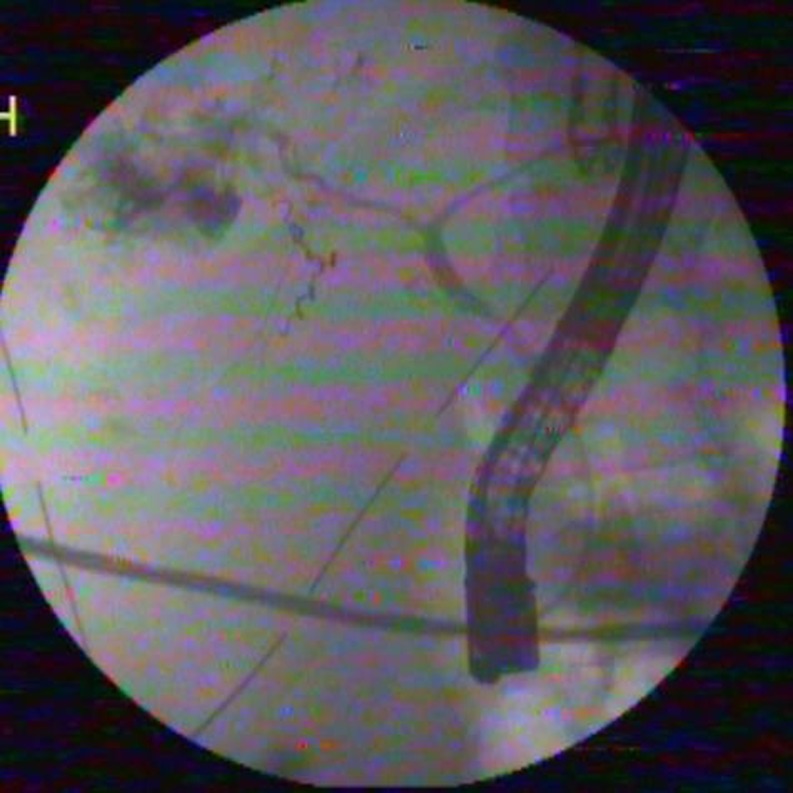
Management of massive liver trauma (grades IV-VI) is associated with high morbidity and mortality. It can pose serious challenges to treating physician and requires multimodality interventions. For a successful outcome, timing of intervention is crucial. We report a case of grade V hepatic injury treated successfully with angioembolization, laparoscopic lavage, and endoscopic stenting during a time period from admission to discharge on the 24th day. Angioembolization was performed at admission after resuscitation as CT scan showed active extravasation in the arterial phase. Laparoscopic lavage and drainage was performed on the fifth day as abdominal inflammatory response failed to respond to medical management. There was biliary component of abdominal fluid noticed during laparoscopy, which manifested by postoperative localized biliary fistula; hence endoscopic stenting of the bile duct was performed on the seventh day. The patient recovered well with timely minimal invasive approach and was fine at 1 year follow-up.
Keywords: Angiographic embolization; Biliary fistula; Hepatic trauma; Laparoscopic lavage.
Figures





References
-
- Croce MA, Fabian TC, Menke PG, Waddle-Smith L, Minard G, Kudsk KA, et al. Nonoperative management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients. Results of a prospective trial. Ann Surg. 1995;221:744–755. doi: 10.1097/00000658-199506000-00013. - DOI - PMC - PubMed
-
- Cresswell AB, Bowles MJ, Wendon JA (2007) The management of liver trauma. In: Vincent JL (ed) Yearbook of intensive care and emergency medicine, 1st edn. Springer, Berlin, pp 666–77.
LinkOut - more resources
Full Text Sources