

Prevalence and burden of breathlessness in patients with chronic obstructive pulmonary disease managed in primary care
- PMID: 24427316
- PMCID: PMC3888425
- DOI: 10.1371/journal.pone.0085540
Prevalence and burden of breathlessness in patients with chronic obstructive pulmonary disease managed in primary care
Abstract
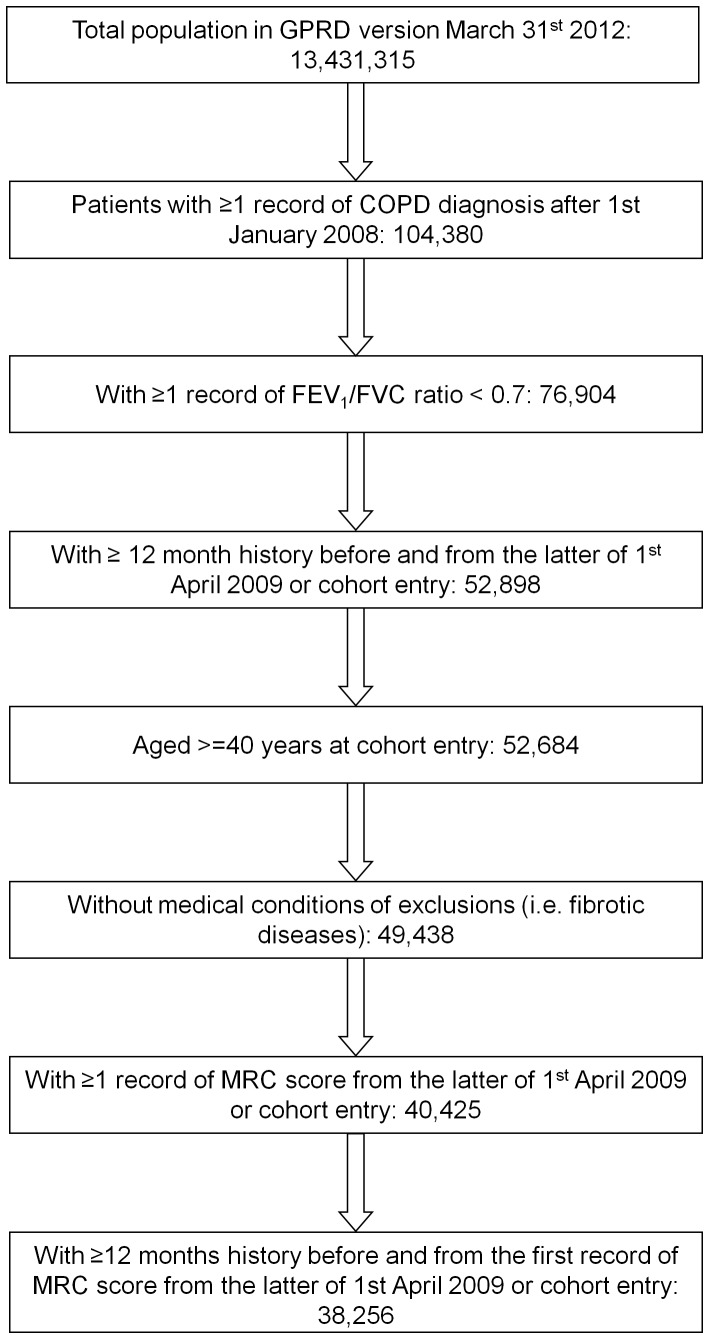
Background & aims: Breathlessness is a primary clinical feature of chronic obstructive pulmonary disease (COPD). We aimed to describe the frequency of and factors associated with breathlessness in a cohort of COPD patients identified from the Clinical Practice Research Datalink (CPRD), a general practice electronic medical records database.
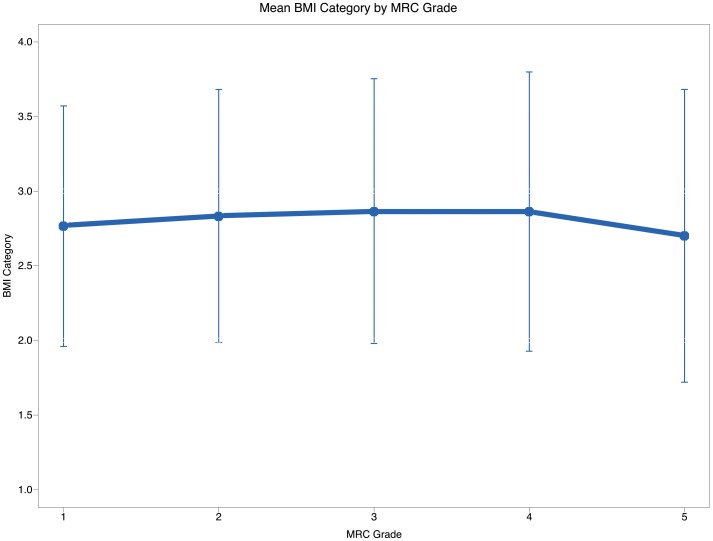
Methods: Patients with a record of COPD diagnosis after January 1 2008 were identified in the CPRD. Breathlessness was assessed using the Medical Research Council (MRC) dyspnoea scale, with scoring ranging from 1-5, which has been routinely administered as a part of the regular assessment of patients with COPD in the general practice since April 2009. Stepwise multivariate logistic regression estimated independent associations with dyspnoea. Negative binomial regression evaluated a relationship between breathlessness and exacerbation rate during follow-up.
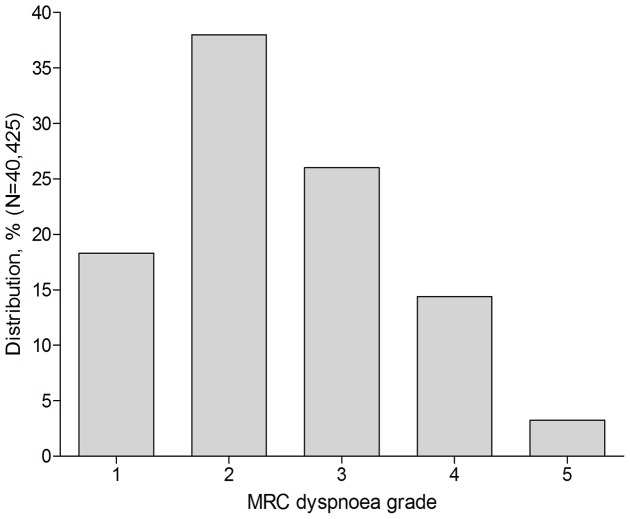
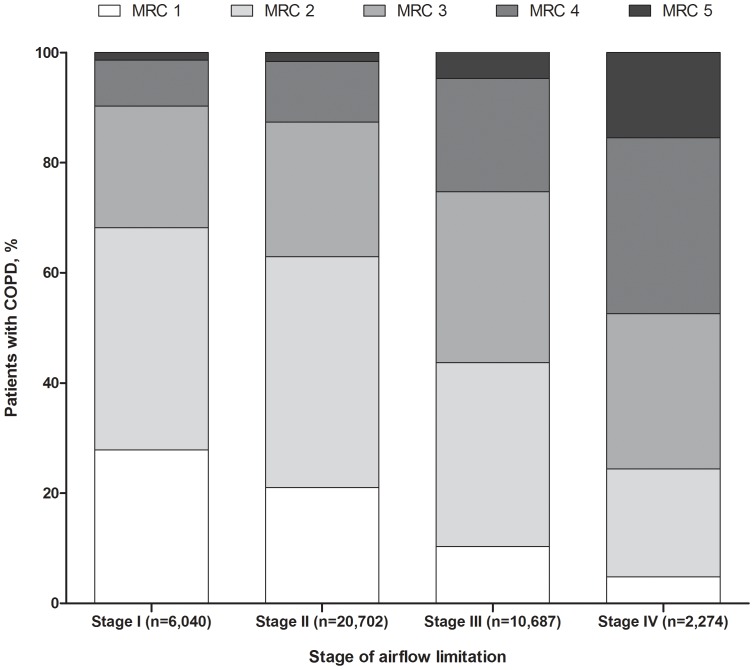
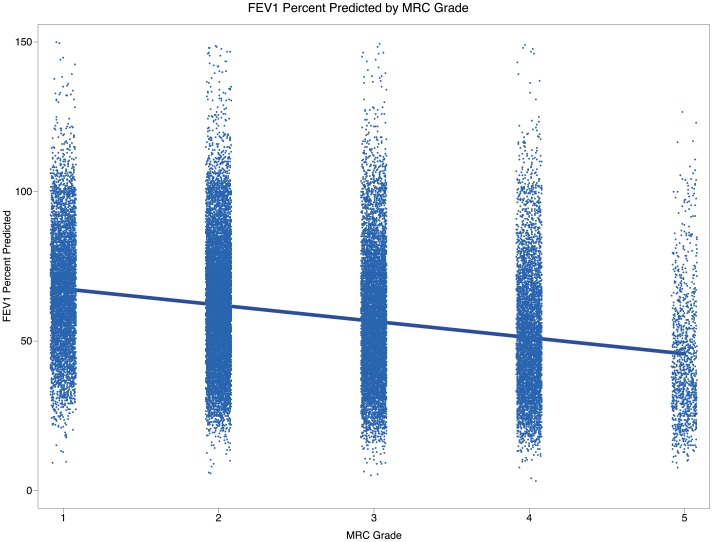
Results: The total cohort comprised 49,438 patients diagnosed with COPD; 40,425 (82%) had any MRC dyspnoea grade recorded. Of those, 22,770 (46%) had moderate-to-severe dyspnoea (MRC ≥ 3). Breathlessness increased with increasing airflow limitation; however, moderate-to-severe dyspnoea was also observed in 32% of patients with mild airflow obstruction. Other factors associated with increased dyspnoea grade included female gender, older age (≥ 70 years), obesity (BMI ≥ 30), history of moderate-to-severe COPD exacerbations, and frequent visits to the general practitioner. Patients with worse breathlessness were at higher risk of COPD exacerbations during follow-up.
Conclusions: Moderate-to-severe dyspnoea was reported by >40% of patients diagnosed with COPD in primary care. Presence of dyspnoea, including even a perception of mild dyspnoea (MRC = 2), was associated with increased disease severity and a higher risk of COPD exacerbations during follow-up.
Conflict of interest statement
Figures
References
-
- Gold Initiative for Chronic Obstructive Lung Disease. (2011) Global strategy for diagnosis, management, and prevention of COPD. Available: http://www goldcopd org/guidelines-global-strategy-for-diagnosis-management html. Accessed 3rd December 2012.
-
- Sarkar S, Amelung PJ (2006) Evaluation of the dyspneic patient in the office. Prim Care 33(3): 643–657. - PubMed
-
- Jolley CJ, Moxham J (2009) A physiological model of patient-reported breathlessness during daily activities in COPD. Eur Respir Rev 18(112): 66–79. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
