

Emerging techniques for dose optimization in abdominal CT
- PMID: 24428277
- PMCID: PMC4319522
- DOI: 10.1148/rg.341135038
Emerging techniques for dose optimization in abdominal CT
Abstract
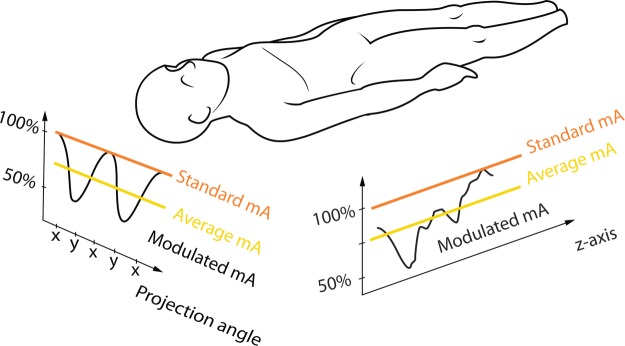
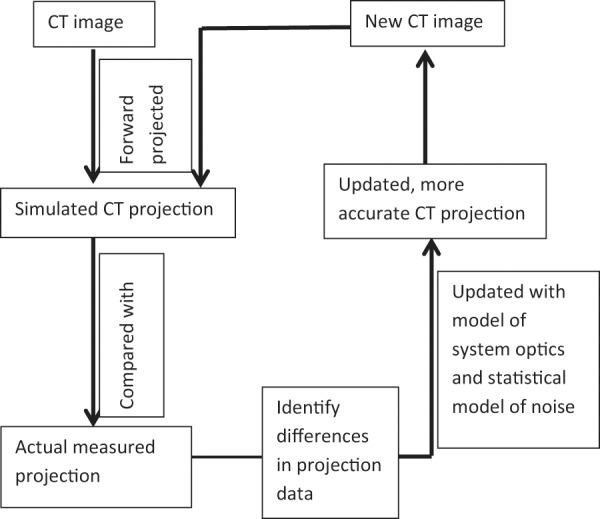
Recent advances in computed tomographic (CT) scanning technique such as automated tube current modulation (ATCM), optimized x-ray tube voltage, and better use of iterative image reconstruction have allowed maintenance of good CT image quality with reduced radiation dose. ATCM varies the tube current during scanning to account for differences in patient attenuation, ensuring a more homogeneous image quality, although selection of the appropriate image quality parameter is essential for achieving optimal dose reduction. Reducing the x-ray tube voltage is best suited for evaluating iodinated structures, since the effective energy of the x-ray beam will be closer to the k-edge of iodine, resulting in a higher attenuation for the iodine. The optimal kilovoltage for a CT study should be chosen on the basis of imaging task and patient habitus. The aim of iterative image reconstruction is to identify factors that contribute to noise on CT images with use of statistical models of noise (statistical iterative reconstruction) and selective removal of noise to improve image quality. The degree of noise suppression achieved with statistical iterative reconstruction can be customized to minimize the effect of altered image quality on CT images. Unlike with statistical iterative reconstruction, model-based iterative reconstruction algorithms model both the statistical noise and the physical acquisition process, allowing CT to be performed with further reduction in radiation dose without an increase in image noise or loss of spatial resolution. Understanding these recently developed scanning techniques is essential for optimization of imaging protocols designed to achieve the desired image quality with a reduced dose.
© RSNA, 2014.
Figures












Comment in
-
Invited commentary.Radiographics. 2014 Jan-Feb;34(1):17-8. doi: 10.1148/rg.341135177. Radiographics. 2014. PMID: 24428278 No abstract available.
Similar articles
-
Assessment of image quality on effects of varying tube voltage and automatic tube current modulation with hybrid and pure iterative reconstruction techniques in abdominal/pelvic CT: a phantom study.Invest Radiol. 2013 Mar;48(3):167-74. doi: 10.1097/RLI.0b013e31827b8f61. Invest Radiol. 2013. PMID: 23344519
-
Successful Dose Reduction Using Reduced Tube Voltage With Hybrid Iterative Reconstruction in Pediatric Abdominal CT.AJR Am J Roentgenol. 2015 Aug;205(2):392-9. doi: 10.2214/AJR.14.12698. AJR Am J Roentgenol. 2015. PMID: 26204293
-
Low-dose abdominal CT: comparison of low tube voltage with moderate-level iterative reconstruction and standard tube voltage, low tube current with high-level iterative reconstruction.Clin Radiol. 2013 Oct;68(10):1008-15. doi: 10.1016/j.crad.2013.04.008. Epub 2013 Jun 21. Clin Radiol. 2013. PMID: 23796210 Clinical Trial.
-
Iterative Reconstruction Techniques in Abdominopelvic CT: Technical Concepts and Clinical Implementation.AJR Am J Roentgenol. 2015 Jul;205(1):W19-31. doi: 10.2214/AJR.14.13402. AJR Am J Roentgenol. 2015. PMID: 26102414 Review.
-
CT radiation dose and iterative reconstruction techniques.AJR Am J Roentgenol. 2015 Apr;204(4):W384-92. doi: 10.2214/AJR.14.13241. AJR Am J Roentgenol. 2015. PMID: 25794087 Review.
Cited by
-
Emerging clinical applications of computed tomography.Med Devices (Auckl). 2015 Jun 5;8:265-78. doi: 10.2147/MDER.S70630. eCollection 2015. Med Devices (Auckl). 2015. PMID: 26089707 Free PMC article. Review.
-
Contrast media and radiation dose optimization with task-based automatic keV selection: a proof-of-concept study with photon-counting detector CT.Eur Radiol. 2025 Jun 12. doi: 10.1007/s00330-025-11738-3. Online ahead of print. Eur Radiol. 2025. PMID: 40506637
-
Triple-phase abdomen and pelvis computed tomography: standard unenhanced phase can be replaced with reduced-dose scan.Pol J Radiol. 2018 Apr 22;83:e166-e170. doi: 10.5114/pjr.2018.75682. eCollection 2018. Pol J Radiol. 2018. PMID: 30627230 Free PMC article.
-
CT imaging of congenital lung lesions: effect of iterative reconstruction on diagnostic performance and radiation dose.Pediatr Radiol. 2015 Jul;45(7):989-97. doi: 10.1007/s00247-015-3281-4. Epub 2015 Jan 31. Pediatr Radiol. 2015. PMID: 25636530
-
Deep learning reconstruction improves image quality of abdominal ultra-high-resolution CT.Eur Radiol. 2019 Nov;29(11):6163-6171. doi: 10.1007/s00330-019-06170-3. Epub 2019 Apr 11. Eur Radiol. 2019. PMID: 30976831
References
-
- Sodickson A, Baeyens PF, Andriole KP, et al. Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology. 2009;251(1):175–184. - PubMed
-
- Health Physics Society. Radiation risk in perspective: position statement of the Health Physics Society. http://www.hps.org/documents/radiationrisk.pdf. Revised August 2004. Accessed May 20, 2013.
-
- Mettler FA, Jr, Bhargavan M, Faulkner K, et al. Radiologic and nuclear medicine studies in the United States and worldwide: frequency, radiation dose, and comparison with other radiation sources—1950–2007. Radiology. 2009;253(2):520–531. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
