

The effect of social deprivation on clinical outcomes and the use of treatments in the UK cystic fibrosis population: a longitudinal study
- PMID: 24429092
- PMCID: PMC3878382
- DOI: 10.1016/S2213-2600(13)70002-X
The effect of social deprivation on clinical outcomes and the use of treatments in the UK cystic fibrosis population: a longitudinal study
Abstract
Background: Poorer socioeconomic circumstances have been linked with worse outcomes in cystic fibrosis. We assessed whether a relation exists between social deprivation and individual's clinical and health-care outcomes.
Methods: We did a longitudinal registry study of the UK cystic fibrosis population younger than 40 years (8055 people with 49337 observations for weight, the most commonly collected outcome, between Jan 1, 1996, and Dec 31, 2009). We assessed data for weight, height, body-mass index, percent predicted forced expiratory volume in 1 s (%FEV1), risk of Pseudomonas aeruginosa colonisation, and the use of major cystic fibrosis treatment modalities. We used mixed effects models to assess the association between small-area deprivation and clinical and health-care outcomes, adjusting for clinically important covariates. We give continuous outcomes as mean differences, and binary outcomes as odds ratios, comparing extremes of deprivation quintile.
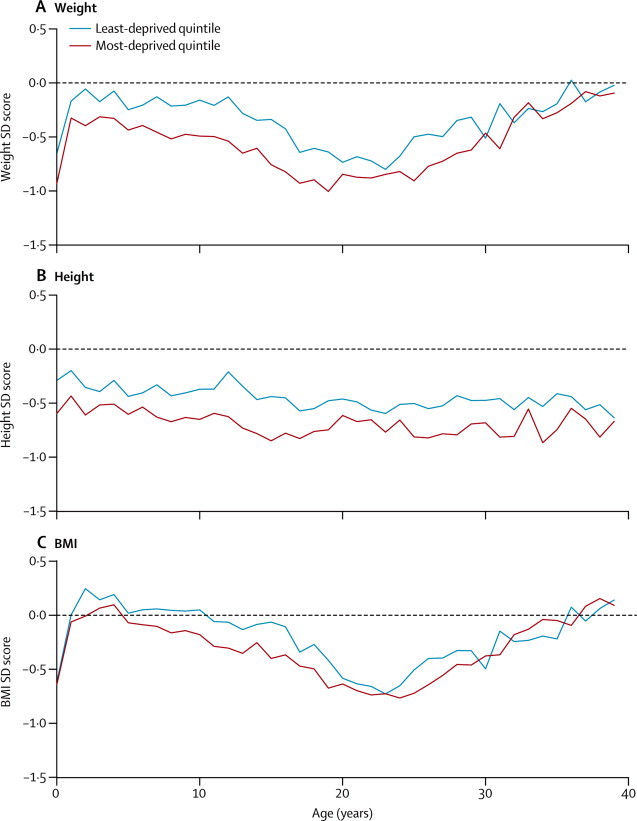
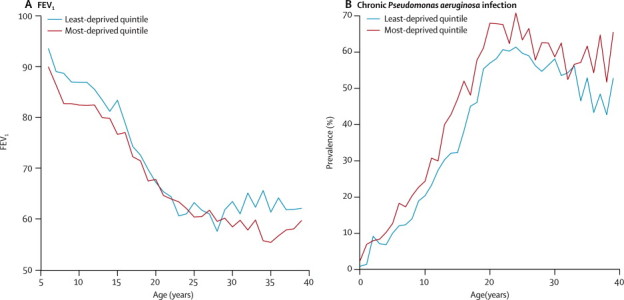
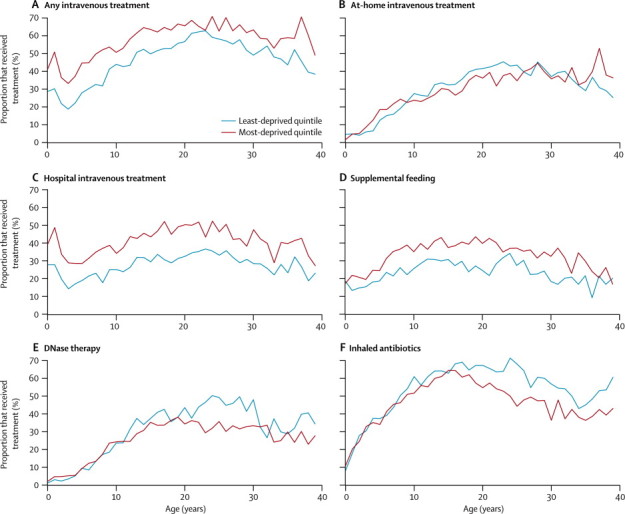
Findings: Compared with the least deprived areas, children from the most deprived areas weighed less (standard deviation [SD] score -0·28, 95% CI -0·38 to -0·18), were shorter (-0·31, -0·40 to -0·21, and had a lower body-mass index (-0·13, -0·22 to -0·04), were more likely to have chronic P aeruginosa infection (odds ratio 1·89, 95% CI 1·34 to 2·66), and have a lower %FEV1 (-4·12 percentage points, 95% CI -5·01 to -3·19). These inequalities were apparent very early in life and did not widen thereafter. On a population level, after adjustment for disease severity, children in the most deprived quintile were more likely to receive intravenous antibiotics (odds ratio 2·52, 95% CI 1·92 to 3·17) and nutritional treatments (1·78, 1·44 to 2·20) compared with individuals in the least deprived quintile. Patients from the most disadvantaged areas were less likely to receive DNase or inhaled antibiotic treatment.
Interpretation: In the UK, children with cystic fibrosis from more disadvantaged areas have worse growth and lung function compared with children from more affluent areas, but these inequalities do not widen with advancing age. Clinicians consider deprivation status, as well as disease status, when making decisions about treatments, and this might mitigate some effects of social disadvantage.
Funding: Medical Research Council (UK).
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Wealth as a disease modifier in cystic fibrosis.Lancet Respir Med. 2013 Apr;1(2):93-5. doi: 10.1016/S2213-2600(13)70014-6. Epub 2013 Feb 1. Lancet Respir Med. 2013. PMID: 24429076 No abstract available.
References
-
- Cystic Fibrosis Trust UK CF Registry annual data report 2010. http://www.cftrust.org.uk/aboutcf/publications/cfregistryreports/ (accessed Sept 28, 2012).
-
- Schechter MS, Shelton BJ, Margolis PA, Fitzsimmons SC. The association of socioeconomic status with outcomes in cystic fibrosis patients in the United States. Am J Respir Crit Care Med. 2001;163:1331–1337. - PubMed
-
- O'Connor GT, Quinton HB, Kneeland T. Median household income and mortality rate in cystic fibrosis. Pediatrics. 2003;111:e333–e339. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
