

Polygenic risk and the development and course of asthma: an analysis of data from a four-decade longitudinal study
- PMID: 24429243
- PMCID: PMC3899706
- DOI: 10.1016/S2213-2600(13)70101-2
Polygenic risk and the development and course of asthma: an analysis of data from a four-decade longitudinal study
Abstract
Background: Genome-wide association studies (GWAS) have discovered genetic variants that predispose individuals to asthma. To integrate these new discoveries with emerging models of asthma pathobiology, we aimed to test how genetic discoveries relate to developmental and biological characteristics of asthma.
Methods: In this prospective longitudinal study, we investigated a multilocus profile of genetic risk derived from published GWAS of asthma case status. We then tested associations between this genetic risk score and developmental and biological characteristics of asthma in participants enrolled in a population-based long-running birth cohort, the Dunedin Multidisciplinary Health and Development Study (n=1037). We used data on asthma onset, asthma persistence, atopy, airway hyper-responsiveness, incompletely reversible airflow obstruction, and asthma-related school and work absenteeism and hospital admissions obtained during nine prospective assessments spanning the ages of 9 to 38 years. Analyses included cohort members of European descent from whom genetic data had been obtained.
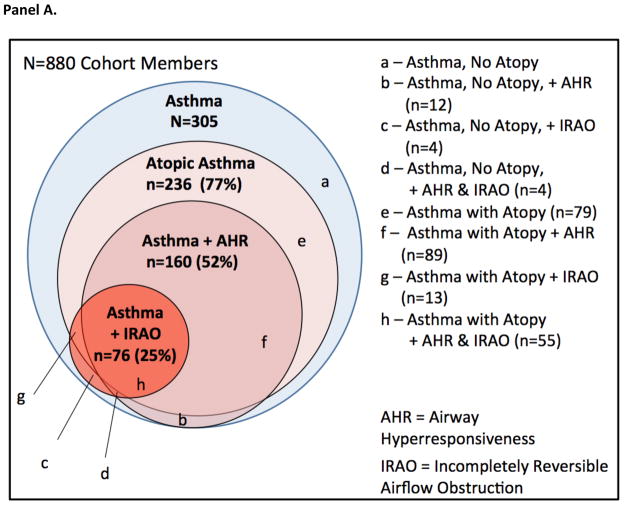
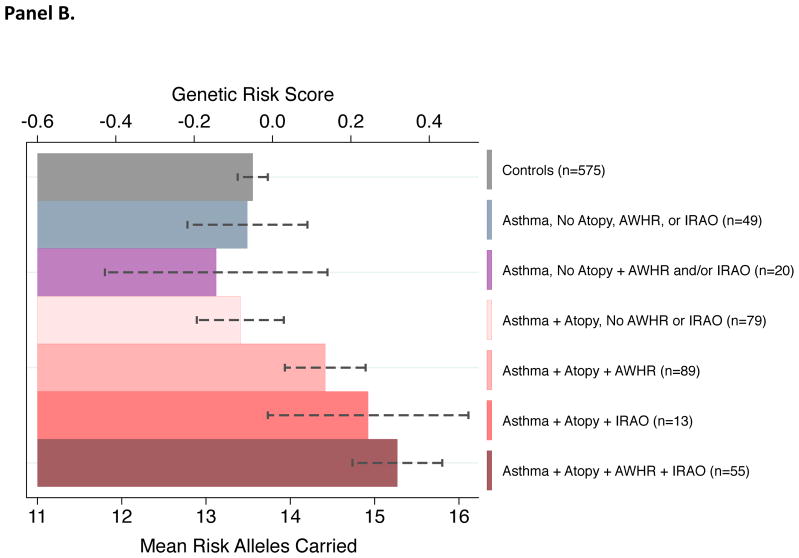
Findings: Of the 880 cohort members included in our analysis, those at higher genetic risk developed asthma earlier in life than did those with lower genetic risk (hazard ratio [HR] 1·12, 95% CI 1·01-1·26). Of cohort members with childhood-onset asthma, those with higher genetic risk were more likely to develop life-course-persistent asthma than were those with a lower genetic risk (relative risk [RR] 1·36, 95% CI 1·14-1·63). Participants with asthma at higher genetic risk more often had atopy (RR 1·07, 1·01-1·14), airway hyper-responsiveness (RR 1·16, 1·03-1·32), and incompletely reversible airflow obstruction (RR 1·28, 1·04-1·57) than did those with a lower genetic risk. They were also more likely to miss school or work (incident rate ratio 1·38, 1·02-1·86) and be admitted to hospital (HR 1·38, 1·07-1·79) because of asthma. Genotypic information about asthma risk was independent of and additive to information derived from cohort members' family histories of asthma.
Interpretation: Our findings confirm that GWAS discoveries for asthma are associated with a childhood-onset phenotype. Genetic risk assessments might be able to predict which childhood-onset asthma cases remit and which become life-course-persistent, who might develop impaired lung function, and the burden of asthma in terms of missed school and work and hospital admissions, although these predictions are not sufficiently sensitive or specific to support immediate clinical translation.
Funding: US National Institute on Aging and UK Medical Research Council.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures


Comment in
-
Can genes forecast asthma risk?Lancet Respir Med. 2013 Aug;1(6):425-6. doi: 10.1016/S2213-2600(13)70143-7. Epub 2013 Aug 5. Lancet Respir Med. 2013. PMID: 24429227 No abstract available.
References
-
- Sears MR. Descriptive epidemiology of asthma. Lancet. 1997;350(Suppl 2):SII1–4. - PubMed
-
- Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012;18:716–25. - PubMed
-
- Zhang YM, Moffatt MF, Cookson WOC. Genetic and genomic approaches to asthma: new insights for the origins. Curr Opin Pulm Med. 2012;18:6–13. - PubMed
-
- Bonfield TL, Ross KR. Asthma heterogeneity and therapeutic options from the clinic to the bench. Curr Opin Allergy Clin Immunol. 2012;12:60–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
